Play all audios:
Sir, Silicone oil is toxic to the cornea causing endothelial failure and band keratopathy.1 In traumatic aniridia and aphakia, there lacks a barrier for silicone oil between the posterior
and anterior chambers. Therefore, if retinal surgery is also required, silicone oil tamponade may cause the cornea to decompensate unless an artificial barrier can be constructed. We report
a novel technique in a patient following globe rupture. CASE REPORT A 43-year-old male who had previous penetrating keratoplasty for keratoconus endured blunt trauma to his left eye. He had
total iris loss and required a repeat penetrating keratoplasty and lensectomy due to the globe rupture. Three weeks later, he had a total retinal detachment with severe proliferative
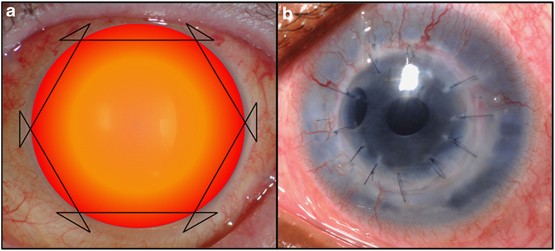
vitreoretinopathy (PVR). He underwent pars plana vitrectomy, retinectomy, PVR membrane peel, laser, and silicone oil tamponade. Before silicone oil injection, 360-degree conjunctival
peritomy was performed, and an artificial barrier was formed using a continuous 10/0 prolene suture (Ethicon W1713, Somerville, NJ, USA) placed 2.5 mm from the corneal limbus (Figure 1a).
Within 2 months, he developed a membrane at the level of the retention suture, seperating the silicone oil from the anterior chamber. Laser capsulotomy was initially planned, but he
subsequently spontaneously developed a central opening within the membrane (Figure 1b). His retina remained flat under oil, and visual acuity at 4 months follow-up was counting fingers.
DISCUSSION Retention sutures are effective in preventing corneal decompensation in aniridic eyes requiring silicone oil tamponade.2 This is because of the surface tension of silicone oil and
its propensity to stay as a single bubble within the vitreous cavity. The method described above allows for one continuous suture to be used in forming the barrier, and is an alternative to
the previously described technique using multiple sutures. It is not known if the hexagonal shape is better than others at stimulating peri-silicone proliferation and membrane formation,3
the rate of which may also vary between patients and with topical steroid use. In our case, an opening in the membrane formed spontaneously, but in others, laser capsulotomy may be required.
REFERENCES * Sternberg P, Hatchell DL, Foulks GN, Landers MB . The effect of silicone oil on the cornea. _Arch Ophthalmol_ 1985; 103 (1): 90–94. Article CAS Google Scholar * Ronald C,
Gentile RC, Eliott D . Silicone oil retention sutures in aphakic eyes with iris loss. _Arch Ophthalmol_ 2010; 128 (12): 1596–1599. Article Google Scholar * Asaria RHY, Kon CH, Bunce C,
Sethi CS, Limb GA, Khaw PT _et al_. Silicone oil concentrates fibrogenic growth factors in the retro-oil fluid. _Br J Ophthalmol_ 2004; 88: 1439–1442. Article CAS Google Scholar Download
references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of Ophthalmology, St. Thomas’ Hospital, London, UK R Wong, E J K Lee & M Shunmugam Authors * R Wong View author
publications You can also search for this author inPubMed Google Scholar * E J K Lee View author publications You can also search for this author inPubMed Google Scholar * M Shunmugam View
author publications You can also search for this author inPubMed Google Scholar CORRESPONDING AUTHOR Correspondence to M Shunmugam. ETHICS DECLARATIONS COMPETING INTERESTS The authors
declare no conflict of interest. RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Wong, R., Lee, E. & Shunmugam, M. Novel technique for silicone oil
retention suture with secondary auto capsulotomy of fibrin membrane. _Eye_ 27, 280–281 (2013). https://doi.org/10.1038/eye.2012.266 Download citation * Published: 14 December 2012 * Issue
Date: February 2013 * DOI: https://doi.org/10.1038/eye.2012.266 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a
shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative