Play all audios:
Care pathways for ST-segment elevation myocardial infarction (STEMI) were interrupted during the coronavirus disease 2019 (COVID-19) pandemic. A new cardiac MRI study has revealed that
increased total ischaemic time for patients with STEMI during major public health restrictions was associated with increased infarct size and other markers of myocardial damage. _Refers to_
Lechner, I. et al. Impact of COVID-19 pandemic restrictions on ST-elevation myocardial infarction: a cardiac magnetic resonance imaging study. _Eur. Heart J_.
https://doi.org/10.1093/eurheartj/ehab621 (2021). The reorganization of health-care services and the implementation of major public health restrictions during the coronavirus disease 2019
(COVID-19) pandemic reduced mortality and morbidity that was directly related to the contagion, but indirectly resulted in ‘collateral damage’ by interrupting care pathways for diseases
other than COVID-19. ST-segment elevation myocardial infarction (STEMI) is a cardiovascular emergency that requires timely reperfusion, typically by means of primary percutaneous coronary
intervention (PPCI). Optimal provision of PPCI is dependent on the implementation of ‘hub’ and ‘spoke’ networks of hospitals linked by a prioritized and efficient ambulance service1.
International reports pertaining to admission of patients with STEMI to hospital during the pandemic described increased mortality after PPCI and longer durations between the time of symptom
onset and treatment2. The MARINA-STEMI cardiac MRI study3 is the latest report on the myocardial tissue damage characteristics of patients with STEMI who were admitted to a hospital during
the COVID-19 pandemic. The prospective MARINA-STEMI cohort study, which involves patients presenting with STEMI to a regional PPCI centre in Austria, provides mechanistic insights regarding
the effect of major public health restrictions on the extent of myocardial tissue damage in these patients3. In this study, patients who were clinically stable after a STEMI underwent
cardiac MRI between three and five days after the myocardial infarction event. The investigators compared 48 patients treated during periods in 2020 when major public health restrictions
were implemented with 101 patients treated during periods in 2020 without public health restrictions and 124 patients treated during the corresponding periods between 2015 and 2019
(pre-pandemic). The investigators used cardiac MRI findings to assess infarct size, defined as percentage of the entire left ventricular myocardial mass, as well as the frequency and extent
of microvascular obstruction and intramyocardial haemorrhage. Each of these markers of myocardial damage has prognostic relevance: a 5% increase in infarct size as measured by cardiac MRI
contributes to a 19% increase in all-cause mortality at one year4. Furthermore, microvascular obstruction is strongly associated with mortality and hospitalization for heart failure within
one year5 and intramyocardial haemorrhage is associated with persistent iron in the infarct core, which is predictive of adverse cardiac remodelling and worsening cardiac function6. Notably,
baseline patient demographics and comorbidity profiles did not differ significantly between groups, and neither did periprocedural or procedural factors such as pharmacological therapy,
frequency of coronary stenting or the frequency of thrombolysis in myocardial infarction (TIMI) flow 3 after PPCI3. However, during periods with major public health restrictions, the median
total ischaemic time in admitted patients was 75 min longer and the proportion of patients with TIMI flow 0 before PPCI was 19% higher than during periods without restrictions3. In addition,
patients treated during periods of major public health restrictions had more deleterious findings on cardiac MRI than patients in the other groups, including a larger infarct size, more
frequent and larger extent of microvascular obstruction, and more frequent intramyocardial haemorrhage. The relationship between myocardial ischaemic time and adverse myocardial function has
been well established for more than 50 years7. Although the present study is only observational and causation cannot be inferred, the data add to mounting evidence of the adverse
population-level effects associated with delayed times between symptom onset and treatment of STEMI during the COVID-19 pandemic2. Moreover, the study investigators are likely to have
underestimated the consequences of interruptions of STEMI care pathways during the pandemic because they did not include patients who were positive for COVID-19, patients who were clinically
unstable after PPCI and the many individuals with acute MI who died in the community8,9. So what does this study add to our knowledge base? Although there is evidence that public mandates
to ‘lock down’ and the resulting delays in seeking help have resulted in excess deaths, this study describes a potential mechanism by which patients with STEMI were subjected to a higher
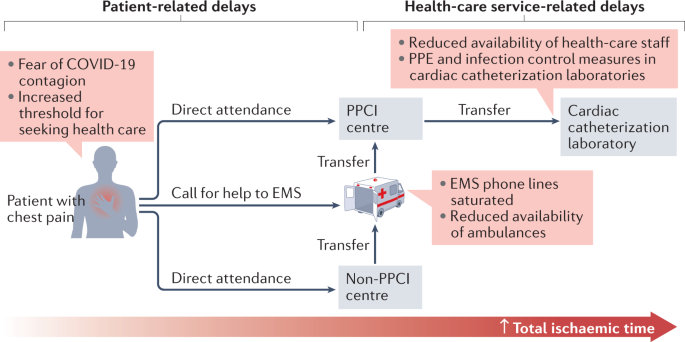
risk of major adverse cardiovascular events despite receiving guideline-recommended care. This observation highlights the importance of addressing the continuum of care for STEMI, including
symptom onset, first medical contact, and ambulance transport and transfer1 (Fig. 1). The health-care pathway relies on communication and process flows between multiple teams across
pre-hospital and hospital settings and thus was particularly vulnerable to the rapid reorganization and overload of health-care services during the pandemic. > The scale of disruption to
STEMI care pathways was not fully > anticipated before the pandemic As we enter a new era of ‘living with’ COVID-19, research demonstrating possible ways to avoid collateral
cardiovascular damage during future waves of infection will have immediate utility. The scale of disruption to STEMI care pathways was not fully anticipated before the pandemic, and might
have been exacerbated by policies and communication strategies. During the initial stages of the pandemic, patients feared the potential COVID-19 contagion and did not wish to add additional
workload to health-care services that were viewed to be under severe strain. Coordinated regional campaigns from cardiovascular societies, charities and public health institutions to raise
awareness of the importance of seeking medical attention for symptoms of MI have resulted in faster normalization of hospital attendance rates for MI to pre-pandemic levels compared to
regions where no such campaigns were conducted10. Furthermore, pre-hospital networks might need to be fortified, especially in low-income and middle-income countries, to ensure that patients
arrive expediently at PPCI centres for treatment. Going forward, health-care services will need to create additional capacity to manage the morbidity that will arise from extra myocardial
tissue damage sustained by patients with delayed treatment for STEMI during the pandemic, and plan to protect existing STEMI care pathways in the event of future waves of COVID-19-related
infection. REFERENCES * Kontos, M. C. et al. Prehospital activation of hospital resources (PreAct) ST-segment–elevation myocardial infarction (STEMI): a standardized approach to prehospital
activation and direct to the catheterization laboratory for STEMI recommendations from the American Heart Association’s Mission: Lifeline Program. _J. Am. Heart Assoc._ 9, e011963 (2020).
Article CAS Google Scholar * Chew, N. W. et al. The global impact of the COVID-19 pandemic on STEMI care: a systematic review and meta-analysis. _Can. J. Cardiol._ 37, 1450–1459 (2021).
Article Google Scholar * Lechner, I. et al. Impact of COVID-19 pandemic restrictions on ST-elevation myocardial infarction: a cardiac magnetic resonance imaging study. _Eur. Heart J._
https://doi.org/10.1093/eurheartj/ehab621 (2021). Article PubMed Google Scholar * Stone, G. W. et al. Relationship between infarct size and outcomes following primary PCI: patient-level
analysis from 10 randomized trials. _J. Am. Coll. Cardiol._ 67, 1674–1683 (2016). Article Google Scholar * de Waha, S. et al. Relationship between microvascular obstruction and adverse
events following primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: an individual patient data pooled analysis from seven randomized trials. _Eur.
Heart J._ 38, 3502–3510 (2017). Article Google Scholar * Carberry, J. et al. Persistent iron within the infarct core after ST-segment elevation myocardial infarction: implications for left
ventricular remodeling and health outcomes. _JACC Cardiovasc. Imaging_ 11, 1248–1256 (2018). Article Google Scholar * Maroko, P. R. et al. Factors influencing infarct size following
experimental coronary artery occlusions. _Circulation_ 43, 67–82 (1971). Article CAS Google Scholar * Wu, J. et al. Place and underlying cause of death during the COVID-19 pandemic:
retrospective cohort study of 3.5 million deaths in England and Wales, 2014 to 2020. _Mayo Clin. Proc._ 96, 952–963 (2021). Article CAS Google Scholar * Wu, J. et al. Place and causes of
acute cardiovascular mortality during the COVID-19 pandemic. _Heart_ 107, 113–119 (2021). Article CAS Google Scholar * Van Belle, E. et al. Myocardial infarction incidence during national
lockdown in two French provinces unevenly affected by COVID-19 outbreak: an observational study. _Lancet Reg. Health Eur._ 2, 100030 (2021). Article Google Scholar Download references
AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Leeds Institute for Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, UK Ramesh Nadarajah & Chris P. Gale * Department of
Cardiology, Leeds Teaching Hospitals NHS Trust, Leeds, UK Ramesh Nadarajah & Chris P. Gale Authors * Ramesh Nadarajah View author publications You can also search for this author
inPubMed Google Scholar * Chris P. Gale View author publications You can also search for this author inPubMed Google Scholar CORRESPONDING AUTHOR Correspondence to Ramesh Nadarajah. ETHICS
DECLARATIONS COMPETING INTERESTS The authors declare no competing interests. RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Nadarajah, R., Gale, C.P.
Collateral cardiovascular damage during the COVID-19 pandemic. _Nat Rev Cardiol_ 19, 81–82 (2022). https://doi.org/10.1038/s41569-021-00661-x Download citation * Published: 02 December 2021
* Issue Date: February 2022 * DOI: https://doi.org/10.1038/s41569-021-00661-x SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable
link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative