Play all audios:
ABSTRACT Somatostatin receptors (SST), especially SST2A, are known for their overexpression in well-differentiated gastroenteropancreatic neuroendocrine neoplasms (GEP-NEN). The chemokine
receptor CXCR4, in contrast, is considered to be present mainly in highly proliferative and advanced tumors. However, comprehensive data are still lacking on potential differences in SST or
CXCR4 expression pattern in GEP-NEN in dependence on the place of origin. Overall, 412 samples from 165 GEP-NEN patients, comprising both primary tumors (PT) and metastases (MTS),
originating from different parts of the gastrointestinal tract or the pancreas were evaluated for SST and CXCR4 expression by means of immunohistochemistry using monoclonal antibodies. SST2A
was present in 85% of PT with a high intensity of expression, followed by SST5 (23%), CXCR4 (21%), SST3 (10%), SST1 (9%), and SST4 (4%). PT displayed higher SST2A and chromogranin A (CgA)
expression levels than MTS. In both PT and MTS lower SST2A and CgA expression levels were found in tumors originating from the appendix or colon, compared to tumors from other origins.
Tumors derived from appendix or colon were associated with significantly worse patient outcomes. Positive correlations were noted between SST2A and CgA as well as between CXCR4 and Ki-67
expression levels. SST2A and CgA negativity of the tumors was significantly associated with poor patient outcomes. All in all, SST2A was the most prominent receptor expressed in the GEP-NEN
samples investigated. However, expression levels varied considerably depending on the location of the primary tumor. SIMILAR CONTENT BEING VIEWED BY OTHERS EXPRESSION PREVALENCE AND DYNAMICS
OF GPCR SOMATOSTATIN RECEPTORS 2 AND 3 AS CANCER BIOMARKERS BEYOND NET: A PAIRED IMMUNOHISTOCHEMISTRY APPROACH Article Open access 27 November 2023 SOMATOSTATIN RECEPTOR 2 (SSTR2)
EXPRESSION IS ASSOCIATED WITH BETTER CLINICAL OUTCOME AND PROGNOSIS IN RECTAL NEUROENDOCRINE TUMORS Article Open access 19 February 2024 WELL-DIFFERENTIATED GASTROENTEROPANCREATIC G3 NET:
FINDINGS FROM A LARGE SINGLE CENTRE COHORT Article Open access 09 September 2021 INTRODUCTION Somatostatin receptors (SST), especially SST2A, are well known for their overexpression in
well-differentiated gastroenteropancreatic neuroendocrine neoplasms (GEP-NEN), where they serve as the molecular basis for SST-based diagnostics and treatment modalities. The chemokine
receptor CXCR4, in contrast, is considered to be present mainly in highly proliferative and advanced tumors. In many studies, it has been demonstrated, that elevated CXCR4 expression is
associated with rapid tumor progression, high invasiveness, early metastasis, and poor patient outcome1,2. Recently, it has been shown that SST2A expression gradually declines with
increasing malignancy from G1 neuroendocrine tumors to G3 neuroendocrine carcinomas3,4,5,6,7,8,9,10,11,12,13, whereas CXCR4 expression is increased14,15,16. Correspondingly, in GEP-NEN SST2A
positivity of the tumor has been associated with better patient outcome3,6,8,9,10,12,17, whereas presence of CXCR4 has been related to low overall survival15. Apart from that, it has been
suggested that malignancy as well as overall survival rates may differ depending on the localization of the GEP-NEN along the gastrointestinal tract, with higher malignancy (Ki-67 levels)
and thus lower survival rates in hindgut as compared to foregut tumors18. Since such distinctions have implications for diagnostic and therapeutic procedures, it would be of interest to know
if there are also differences in SST or CXCR4 expression patterns in GEP-NEN of different anatomical origin. Due to the scarcity of GEP-NEN cases comprehensive data on this issue are still
lacking. Therefore, the aim of the present study was to re-evaluate SST and CXCR4 expression in a large set of formalin-fixed, paraffin-embedded GEP-NEN samples originating from stomach,
duodenum/jejunum, ileum, appendix, colon, rectum or pancreas by using well characterized rabbit monoclonal antibodies19,20,21,22,23 and to correlate the expression with clinical data.
METHODS TUMOR SPECIMENS A total of 412 archived formalin-fixed, paraffin-embedded tumor samples from 165 patients (in detail, 61 × 1, 41 × 2, 30 × 3, 20 × 4, 7 × 5, 2 × 6, 2 × 7, 1 × 10, and
2 × 14 samples per patient) with histologically verified gastroenteropancreatic neuroendocrine neoplasm (132 primary tumors, 95 metastases) were included in the present investigation. These
samples are derived from a different cohort of patients as compared to our previous investigation7. Of the tumors, 19 (12%) originated from the stomach, 15 (9%) from the duodenum/jejunum,
59 (36%) from the ileum, 5 (3%) from the appendix, 9 (5%) from the colon, 14 (8%) from the rectum, and 39 (24%) from the pancreas. From 5 tumors (3%) localization of the primary was unknown.
The samples were provided by the Institute of Pathology and Cytology Bad Berka, Bad Berka, Germany, and had been surgically removed between 1999 and 2014 at the Department of General and
Visceral Surgery, Zentralklinik Bad Berka, Bad Berka, Germany. The clinical data were gathered from the patient records. In 82 of the 165 patients an SST-based PET/CT had been performed. The
PET/CT scans were processed with Siemens e.soft Nuclear Medicine Workstation. With the help of this software, automatic region of interest was drawn on the individual tumor lesions and
SUVmax values were calculated. To avoid major influence of partial volume effect on lesion SUVmax, region of interest was drawn only on lesions greater than 1.5 cm in size. Permission was
gained from the local ethics committee (Ethikkommission der Landesärztekammer Thüringen) for this retrospective analysis. All data were recorded and analyzed anonymously.
IMMUNOHISTOCHEMISTRY From the paraffin blocks, 4 µm sections were prepared and floated onto positively charged slides. Immunostaining was performed by an indirect peroxidase labeling method
as described previously24. Rabbit monoclonal antibodies (hybridoma cell culture supernatants) directed against the respective carboxyl-terminal tails of the receptors were used to detect
SSTs (except for SST4) and CXCR4 (for detailed information on the clones, epitopes, and the dilutions of the antibodies, see Supplementary Table 5). With respect to SST4, similar, but
polyclonal, antibodies were applied. Sections from human pancreas (islets; SST1, SST2A, SST3, SST5), lymph nodes (germinal centers; SST2A, SST5, CXCR4), and human cortex (SST4) served as
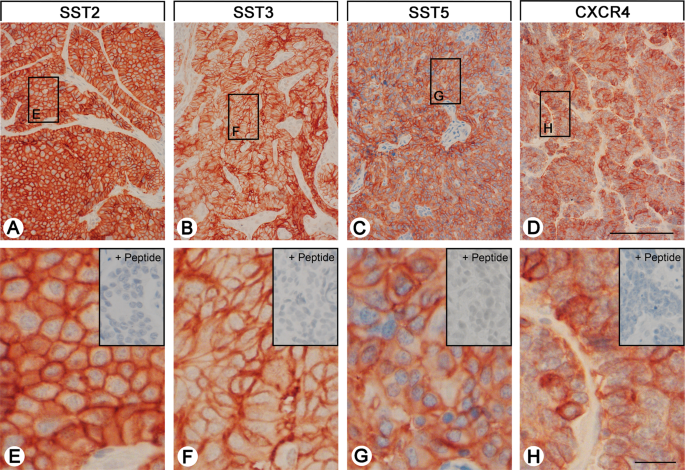
positive controls. As negative control, the primary antibody was either omitted or adsorbed for 2 h at room temperature with 10 µg/ml of the peptide used for immunizations. In all cases a
complete abolition of immunostaining was observed (see insets in Fig. 1 and in Supplementary Fig. 1). Additional stainings were performed with monoclonal mouse antibodies against the
proliferation marker Ki-67 and against chromogranin A (CgA), a marker for neuroendocrine tumors (Supplementary Table 5). Staining for the receptors as well as for CgA in all sections was
scored by means of the semiquantitative Immunoreactivity Score (IRS) according to Remmele and Stegner25. The percentage of positive tumor cells quantified in five gradations (no positive
cells (0), <10% positive cells (1), 10–50% positive cells (2), 51–80% positive cells (3), >80% positive cells (4)) was multiplied by the staining intensity quantified in four
gradations (no staining (0), mild staining (1), moderate staining (2), strong staining (3)). Thus, IRS values ranging from 0 to 12 were obtained. Tumor samples with average IRS values ≥3
were considered positive. With the antibodies against the SSTs and the CXCR4 distinct immunostaining of the plasma membrane, but also of the cytoplasm of the tumor cells was seen, which
reflects receptor internalization due to agonist stimulation. Both types of staining, cytoplasmatic and cell surface staining, were evaluated equally. With respect to Ki-67 staining, the
percentage of positive nuclei was determined. All immunohistochemical stainings were evaluated by two independent blinded investigators (RM, AL). In case of discrepant scores, final decision
was achieved by consensus. STATISTICS For statistical analysis, the IBM SPSS statistics program version 22.0.0.0 was used. Because the data were not normally distributed (Kolmogorov-Smirnov
test), Kruskal-Wallis test, Mann-Whitney test, Chi-Square test, Kendall’s τ-b test, and Spearman’s rank correlation were performed. For survival analysis, the Kaplan-Meier method with a
log-rank test was used. P values ≤ 0.05 were considered statistically significant. In cases where one patient had more than one tumor slide, an arithmetic mean was calculated from the IRS
values of all the slides of this patient, primary tumor and metastasis/es taken together (per patient analysis). Only when primary tumors and metastases were compared, arithmetic means were
calculated for the primary tumor samples and metastasis/es sample(s) separately. ETHICS APPROVAL AND CONSENT TO PARTICIPATE All procedures performed in this study involving human
participants were in accordance with the 1964 Helsinki declaration and its later amendments. Permission was gained from the local ethics committee (Ethikkommission der Landesärztekammer
Thüringen) for this retrospective analysis. Informed consent for the use of tissue samples for scientific purposes was obtained from all individual participants included in the study when
entering the Theranostic Research Center, Zentralklinik Bad Berka, Bad Berka, Germany. All data were analyzed anonymously. RESULTS PATIENT CHARACTERISTICS In total, tumors from 94 male (57%
of the cases) and 71 female patients (43%) were evaluated in the present investigation. Mean age of the patients at diagnosis was 58.8 years overall (median: 59.0 years, range: 12.1–85.0
years), with some differences in dependence on the localization of the primary tumor (Kruskal-Wallis test: p = 0.082; Supplementary Table 1). Patients having tumors originating from the
colon were diagnosed at a significantly older age as compared to those with tumors from the stomach, duodenum/jejunum, ileum or pancreas (pairwise Mann-Whitney tests: p < 0.050).
Twenty-three of the (corresponding) primary tumors (14%) were classified as T1, 22 (13%) as T2, 51 (31%) as T3, and 21 (13%) as T4. In 48 cases (29%), the extent of the primary tumor was
unknown. Thirty-six of the patients (22%) had no lymph node metastases, whereas in 101 cases (61%) lymph node metastases were already present. For 28 tumors (17%) lymph node status was not
known. Forty-nine patients (30%) had no distant metastases, in 97 patients (59%) distant metastases were already present, and in 19 cases (11%) the existence of distant metastases was
unknown (Supplementary Table 2). Distant metastases were mainly found in the liver, but were present also in other parts of the gastrointestinal tract or the pancreas, in the peritoneum,
retroperitoneum, omentum, mesenterium, mesocolon, brain, thyroid, lung, gallbladder, lig. hepatoduodenale, spleen, adrenals, fat capsule of the kidney, kidney, ovary, testis, abdominal
adipose tissue, abdominal wall, bones or skin. At diagnosis, 17 patients (10%) had UICC stage I disease, 8 patients (6%) had stage II disease, 23 patients (14%) had stage III disease, and 97
patients (58%) had already stage IV disease. From 20 patients (12%) the stage of the disease was unknown (Supplementary Table 3). With respect to histological grading, 80 patients (48.5%)
had grade 1, 61 patients (37%) had grade 2, and 24 patients (14.5%) displayed grade 3 histology (Supplementary Table 3). Regarding functionality, 101 tumors (61.2%) were non-functional and
62 (37.6%) functional. In 2 cases (1.2%) functionality of the tumor was not reported in the patient files. Median survival was 4.0 years overall (minimum: 0 months, maximum: 29.3 years).
Here, patients with tumors originating from appendix or colon displayed significantly worse outcomes compared to patients with other derivations of the primary tumor (pairwise log-rank
tests: p < 0.05; Supplementary Table 1; Supplementary Fig. 2). Interestingly, this seems to be independent of the presence of lymph node or distant MTS, as e.g. tumors from the ileum
already displayed lymph node MTS in 86% (colon: 77.8%), and distant MTS in 73% (colon: 66.7%) of the cases (Supplementary Table 2). There were, however, significant differences between the
primary tumor localizations regarding tumor size/infiltrating growth and grading (χ2 test: p < 0.001). At diagnosis in stomach, duodenum/jejunum, ileum and rectum pT4 tumors were present
in 11.1%, 27.3%, 17.4%, 0% and 12.1% of the cases and G3 tumors in 15.8%, 6.7%, 0%, 21.4% and 20.5% of the patients, respectively. By contrast, in appendix and colon pT4 tumors were
diagnosed in already 50% of the patients and G3 tumors in 40% and 55.6% of the cases, respectively (Supplementary Tables 2, 3). All data of the individual patients including gender, age,
localisation of the primary tumor, type and derivation of the samples investigated as well as prior therapies are depicted in the Supplementary Table 6. SOMATOSTATIN AND CXCR4 CHEMOKINE
RECEPTOR EXPRESSION PATTERN Figure 1 and Supplementary Fig. 1 show examples of staining with the monoclonal antibodies against SST1, 2A, 3 and 5, and CXCR4. Distinct immunostaining of the
plasma membrane, but also of the cytoplasm of the tumor cells was seen, which may reflect receptor internalization due to agonist stimulation. The polyclonal anti-SST4 antibody, in contrast,
showed only cytoplasmic positivity (Supplementary Fig. 1). Overall, SST2A was by far the most prominently expressed receptor in the GEP-NEN samples investigated (Fig. 2A,B), followed by
SST5, CXCR4, SST3, SST1 and SST4. For all receptors, expression levels varied considerably between individual patients and sometimes also between different samples from the same patient.
This holds true especially for SST2A, where a huge variation was seen in expression levels between different patients, reaching from 0 IRS points (no expression) to 12 IRS points (maximum
expression), which is illustrated by the length of the respective boxes and whiskers in Fig. 2B. To evaluate the extent of intratumor heterogeneity in receptor expression, the mean standard
deviation (SD) of the IRS values of the SSTs and of the CXCR4 was calculated from the respective SDs of the individual patients for all samples (primary tumors plus metastases taken
together) as well as for the primary tumors (PT) and metastases (MTS) separately. Here, the following results were obtained, showing again the highest variation for the SST2A, but also a
similar variation in PT and MTS: Mean SD: SST1: all samples: 1.00, PT: 1.22, MTS: 0.75; SST2A: all samples: 4.21, PT: 4.15, MTS: 4.20; SST3: all samples: 1.47, PT: 1.33, MTS: 1.59; SST4: all
samples: 1.11, PT: 0.86, MTS: 1.30; SST5: all samples: 2.81, PT: 2.80, MTS: 2.83; CXCR4: all samples: 2.24, PT: 2.08, MTS: 2.38. There was a significant positive correlation (p < 0.05)
between SST1 levels and SST3, SST4, SST5 and CXCR4 expression, of SST2A levels and SST3 and SST5 expression, of SST3 levels and SST1, SST4 and SST5 expression, of SST4 levels and SST1, SST3,
SST5 and CXCR4 expression, and of SST5 levels with those of all other receptors investigated. CXCR4 presence correlated positively with SST1, SST4 and SST5 expression (Table 1).
SOMATOSTATIN AND CXCR4 RECEPTOR EXPRESSION IN DEPENDENCE ON TUMOR LOCALIZATION Compared to MTS, PT displayed significantly higher SST2A and Chromogranin A (CgA) expression levels as well as
significantly higher maximum standardized uptake values (SUVmax) in the SST-PET/CT (Mann-Whitney test: SST2A: p = 0.032; CgA: p = 0.041; SUVmax: p = 0.020) (Supplementary Fig. 3). No
significant differences were observed between PT and MTS with respect to expression levels of the other SSTs and CXCR4 and regarding Ki-67 values (Supplementary Fig. 3). Independently of
that, when correlating the IRS values of the SSTs, CXCR4 and CgA, the Ki-67 levels and the SUVmax values of the SST-PET/CT between PT and MTS of the individual patients, significant
interrelationships were found for the SST2A (rsp = 0.627; p < 0.001), the SST4 (rsp = 0.371, p = 0.003), the SST5 (rsp = 0.302, p = 0.016), the CXCR4 (rsp = 0.613, p < 0.001), CgA (rsp
= 0.405, p = 0.001), the Ki-67 index (rsp = 0.767, p < 0.001) and the SUVmax values of the SST-PET/CTs (rsp = 0.371, p = 0.044). When comparing tumors from different provenances,
dissimilarities were seen with respect to SST2A expression, with significantly lower IRS values in tumors originating from colon or appendix than in those from other origins (Kruskal-Wallis
test: p = 0.037; pairwise Mann-Whitney tests: p < 0.05). These differences were also present when considering PT and MTS separately (Kruskal-Wallis test: PT: p = 0.048; MTS: p = 0.055;
pairwise Mann-Whitney tests: PT; MTS: p < 0.05 except for appendix/colon vs. rectum or pancreas) (Fig. 3A). Similar results were obtained also for CgA levels (Kruskal-Wallis test: PT plus
MTS: p < 0.001; PT: p < 0.001; MTS: p = 0.009; pairwise Mann-Whitney tests: p < 0.05) (Fig. 3B). Significant differences were also seen for CXCR4 expression between the various
tumor localizations (Kruskal-Wallis test: PT plus MTS: p = 0.001; PT: p < 0.001; MTS: p = 0.042). However, in this case tumors originating from appendix or colon showed higher CXCR4
expression values than those from other regions (Fig. 4A). In the pairwise comparisons, however, these differences were not statistically significant, except between colon and ileum in PT
(Mann-Whitney test: p = 0.024) and MTS samples (Mann-Whitney test: p = 0.020). Differences were also seen with respect to Ki-67 values (Kruskal-Wallis test: PT plus MTS; PT; MTS: p <
0.001). Also here, tumor samples from appendix and colon tended to higher values compared to those from other provenances. However, in the pairwise comparisons significant differences were
only detected between colon and ileum samples (Mann-Whitney test: PT plus MTS: p = 0.002; PT: p = 0.009; MTS: p = 0.038) (Fig. 4B). With all other parameters investigated no relevant
differences between the different tumor entities were seen. CORRELATIONS WITH CLINICAL DATA CHROMOGRANIN A AND KI-67 EXPRESSION There was a significant positive correlation between CgA and
SST2A and SST3 expression intensities (Table 1) and also between CgA positivity and SST2A positivity (IRS ≥ 3) of the tumors (χ2 test: p < 0.001). Between CgA and CXCR4 expression
intensities, in contrast, a negative association was noted (Table 1). Between the Ki-67 index and SST1, SST5 and CXCR4 expression levels positive correlations were observed, but negative
correlations between the Ki-67 index and the SST2A and CgA score values (Table 1). SST-BASED PET/CT In 82 of the 165 patients (i.e. 50% of the cases) an SST-based Ga-68 PET/CT had been
performed preoperativly; in 66 cases Ga-68 DOTA-TOC [DOTA-D-Phe1-Tyr3-octreotide] was used, in 9 cases Ga-68 DOTA-TATE [DOTA-(Tyr3)-octreotate], and in 6 cases Ga-68 DOTA-NOC
[DOTA-[Nal3]-octreotide]. SUVmax values of the SST-PET/CT scans showed a significant association with the SST2A expression intensities of the tumors, but (though less pronounced) also with
the IRS values for SST1 and SST5 (Table 1). When considering the DOTA-TOC-PET/CT scans separately, a significant interrelationship was seen for SST2A only (rs = 0.450, p < 0.001). TNM
STATUS AND TUMOR STAGING AND GRADING SST5 and CXCR4 as well as Ki-67 expression intensities significantly correlated with tumor grading (SST5: τ = 0.178, p = 0.007; CXCR4: τ = 0.256, p <
0.001; Ki-67: τ = 0.894, p < 0.001), whereas a negative correlation was noted between SST2A and CgA expression intensities and tumor grading (SST2A: τ = −0.281, p < 0.001; CgA: τ =
−0.313, p < 0.005), or tumor size (SST2A: τ = −0.204, p = 0.005; CgA: τ = −0.208, p = 0.005). CgA serum values, in contrast, exhibited a positive association with tumor stage and size
(tumor stage: τ = 0.351, p < 0.001; tumor size: τ = 0.280, p = 0.005). Presence or absence of lymph node or distant MTS had no influence on SST, CXCR4 or CgA expression intensities and
also no effect on SUVmax values of the PET/CT scans. CHROMOGRANIN A SERUM LEVELS AND KARNOFSKY PERFORMANCE INDEX No interrelationship was seen between CgA serum values and CgA expression in
the tumor samples (r = 0.039, p = 0.744). There was also no correlation between serum CgA levels and SST or CXCR4 expression in the tumors. In case of distant metastases, patients showed
significantly higher serum CgA levels (Mann-Whitney test: p < 0.001), a reduced Karnofsky index (Mann-Whitney test: p = 0.017) and lower overall survival times (Mann-Whitney test: p =
0.001). Correspondingly, between serum CgA levels and the Karnofsky performance index a negative association was observed (rs = −0.325, p = 0.007). TUMOR FUNCTIONALITY Regarding
functionality of the tumors, significantly higher CXCR4 expression rates and a tendency towards a higher Ki-67 index were seen in non-functional tumors as compared to functional tumors
(Mann-Whitney test: CXCR4: p = 0.019; Ki-67: p = 0.103). CgA serum values, in contrast, were significantly lower in patients with non-functional tumors (Mann-Whitney test: p = 0.006).
Functionality, however, was significantly more often associated with distant metastases (distant metastases were present in 81% of the cases in functional tumors and in 56% of the cases in
non-functional tumors; χ2 test: p = 0.002). All other parameters did not significantly differ between functional and non-functional tumors, including SST expression, overall survival time or
patient outcome, respectively. PATIENT OVERALL SURVIVAL Patient overall survival showed a positive association with SST2A (but not with any other SST) expression intensity (rs = 0.186, p =
0.025) and there was a significantly better outcome of patients with SST2A-positive compared to SST2A-negative tumors (log-rank test: p < 0.001) (Fig. 5A). Similar results were obtained
when considering PT and MTS separately (PT; MTS: log-rank test: p < 0.001; Supplementary Fig. 4), when calculating the statistics with ileum-NEN or pancreas-NEN patients alone (ileum;
pancreas: log-rank test: p < 0.001; Supplementary Fig. 5) or when considering G1, G2 or G3 tumors, pT3 or pT4 tumors, tumors with or without lymph node MTS (pN0/pN1) or distant MTS
(pM0/pM1), IUCC stage 3 or stage 4 tumors, and functional and non-functional tumors separately (in all cases: log-rank test: p < 0.01). Also when SST2A positive cases were grouped
according to the median IRS value into cases with moderate (IRS ≤8) or strong (IRS >8) SST2A expression, a significantly better patient outcome was seen for the patients with tumors with
strong in comparison to those with neoplasms with moderate SST2A expression (log-rank test: p = 0.005; Supplementary Fig. 6). As with SST2A, significantly better outcomes were also seen in
patients with CgA-positive neoplasms compared to CgA-negative tumors (PT plus MTS, PT and MTS separately: log-rank test: p < 0.001; all other cases log-rank test: p < 0.020) (Fig. 5B).
On the other hand, patient overall survival time and patient outcome were negatively correlated with Ki-67 levels (rs = −0.286, p < 0.001), patient age (rs = −0.258, p = 0.002), tumor
grade (τ = −0.188, p = 0.002; log-rank test: p < 0.001), size (log-rank test: p < 0.001), stage (τ = 0.259, p < 0.001; log-rank test: p < 0.001) and (as mentioned already above)
presence of distant MTS. However, multivariate analysis (including IRS values of SSTs, CXCR4 and CgA, Ki-67 levels, patient age, tumor grade, size and stage, tumor functionality, presence of
lymph node or distant MTS), revealed SST2A expression and Ki-67 levels as the only independent prognostic factors for patient outcome. DISCUSSION The primary aim of the present study was a
comprehensive (re)evaluation of the SST and CXCR4 expression in a large set of GEP-NEN samples of different origin. To the best of our knowledge, the present study represents the largest one
investigating all SST subtypes and CXCR4 by immunohistochemistry using well characterized monoclonal antibodies in different GEP-NEN locations including stomach so far. Furthermore, the
present study is the largest one investigating SST expression in primary tumors and metastases separately. Additionally, in the present study comprehensive correlations of the SST and CXCR4
expression with a broad range of clinical data were performed, which have never been done so far to this extent and in this detail. To the best of our knowledge there are only two studies
available on CXCR4 expression in GEP-NEN so far15,16 comprising 64 and 61 cases, respectively; for an overview of the studies of the last 15 years on SST expression in GEP-NEN, including the
number of cases evaluated, the SSTs studied, the type of antibodies used and if correlations were performed with tumor functionality, location, grading/staging, Ki-67 index, CgA expression,
SST-based imaging or patient outcomes, see Supplementary Table 4. PATIENT CHARACTERISTICS With a median age at diagnosis of 58.5 years and an almost equal gender distribution, our patient
population is very similar to literature data8,17,18,26,27,28,29,30. According to previous reports, GEP-NEN patients are often diagnosed at an already advanced stage of the
disease17,18,28,29. Also in our cohort, 58% of the patients had already stage IV disease at diagnosis, 61% of the cases presented with lymph node MTS, and 59% of the patients had even
distant MTS. Most of our tumor samples were originating from the small intestine (in total 45%), followed by pancreas (24%). Similar frequency distributions of GEP-NEN were also reported by
other authors28,29,31. As observed also in the literature5,10,12,27,28,29, most of the tumors (61.2%) were non-functional, but (as shown also before)29 symptoms were more likely with
metastatic disease. Median survival of our patients was 4.0 years (48 months), which also corresponds to previous findings27,29. Interestingly, and similar to earlier reports18. patients
having tumors originating from appendix or colon displayed a significantly worse outcome than those having tumors from other provenances and patient outcome appears to be dependent on tumor
size/infiltrative growth, metastatic status, stage and grading, as described previously26. SOMATOSTATIN AND CXCR4 CHEMOKINE RECEPTOR EXPRESSION PATTERN In the GEP-NEN samples investigated,
SST2A was by far the most significant SST expressed, followed by SST5 and the other SSTs. These results fit well to recent data obtained in GEP-NEN samples and in pancreatic NEN using
similar monoclonal antibodies as in the present investigation8,15. Whereas strong prevalence of SST2A in GEP-NEN has been shown throughout the literature, regardless of whether polyclonal or
monoclonal antibodies have been used, in many studies higher staining results for the other SSTs have been reported3,4,5,10,32,33,34,35,36. In these studies, however, polyclonal antibodies
were used, which may have led to an over-estimation of expression rates due to their lower specificity. The same holds true for investigations on CXCR4 expression in GEP-NEN, where higher
expression rates were seen with polyclonal antibodies14,16 than with monoclonal ones15. SOMATOSTATIN AND CXCR4 RECEPTOR EXPRESSION IN DEPENDENCE ON TUMOR LOCALIZATION In the present study,
significantly higher SST2A and CgA expression rates as well as SUVmax PET/CT values were observed in PT as compared to MTS, thus confirming previous results15. Additionally and for the first
time, differences in receptor expression could be demonstrated depending on the derivation of the tumor sample. Tumors originating from appendix or colon showed lower SST2A and CgA, but
higher CXCR4 and Ki-67 expression levels as compared to those from other provenances. Fittingly, patients with tumors derived from appendix or colon showed the worst outcome. These
relationships are further substantiated by the fact that in the present study a positive correlation was detected between patient outcome and SST2A or CgA expression, but a negative
association with Ki-67 expression. CORRELATIONS WITH CLINICAL DATA In the present study negative correlations were observed between tumor grading and SST2A and CgA expression, and a positive
association with CXCR4 and Ki-67 expression. Similar relationships with tumor grading have been found previously for SST2A expression3,4,5,6,7,8,9,10,11,12,13, CXCR4 expression7,14,16, and
Ki-67 values3,7,18,31. Regarding SST5 expression, literature data are still conflicting. While in the present study as well as in another investigation5 positive correlations between SST5
expression and tumor grading were found, negative associations have also been reported4,10,12. Due to the overall low expression rates of SST5, further studies with a significantly higher
number of cases are obviously needed. The present study revealed a distinct correlation between SST2A and CgA expression, confirming previous results37. Therefore, CgA expression could be
used as an indirect estimate for SST2A expression levels. Interestingly, there was no interrelationship between tumor CgA expression and serum CgA values. While tumor CgA expression
negatively correlates with tumor size, serum CgA values showed a positive interrelationship with tumor size, presence of distant MTS and tumor stage, thus confirming literature data
demonstrating an association of serum CgA values with tumor burden and patient outcome29,30,38,39,40. In the present study also a distinct correlation between SST2A (but also SST1 and SST5)
expression and SUVmax values in the PET/CT scans was observed. These results further corroborate numerous data in the literature showing good concordance between SST-based imaging modalities
and SST2A (and SST5) expression of the tumors4,15,17,33,34,36,37,41,42. High SST2 expression and high uptake in SST-based imaging represent clinically relevant predictors for potential
success of subsequent pharmacotherapy with somatostatin analogs or for peptide receptor radionuclide therapy (PRRT)43,44,45,46. Regarding the impact of the functionality on malignancy of the
tumors and on patient outcome, literature data are controversial12,47,48,49. In the present investigation, no overt difference between functional and non-functional tumors with respect to
survival rates and patient outcome could be observed. Additionally, as has been shown previously5,32, functionality of the tumors had no influence on SST expression, but there was a
significantly lower CgA expression in non-functional as compared to functional tumors. Furthermore, significantly higher CXCR4 and Ki-67 expression levels in non-functional than in
functional tumors could be shown, pointing to a somewhat higher malignancy of non-functional tumors. The present study also shows a clear-cut positive association between SST2A or CgA
expression and patient outcome/overall survival. Similar observations have been made by several authors3,6,8,9,10,12,17,28, but (due to the high number of cases) we were able to show this
association also for PT and MTS as well as for the different TNM, grading or staging classes or for functional and non-functional tumors separately. We were additionally able to show that
not only SST2A positivity, but also the level of SST2A expression is related to prognosis. Similar to the findings in the present study, no impact of any other SST on the course of the
disease has been found in the literature8,9, with the exception of SST510,12. As expected, Ki-67 levels, tumor size, grade, stage and presence of distant MTS were negatively correlated with
patient outcome/overall survival8,27,28,29. Additionally, patient age was confirmed as a negative predictor27,29. CONCLUSIONS Overall, SST2A was the most prominently expressed receptor in
the GEP-NEN samples investigated. Therefore, SST2A-based functional imaging and (if surgery is not possible) SST2A-based therapies (pharmacotherapy with somatostatin analogs, PRRT) should be
first choice in metastasized tumor stage. Nevertheless, there was substantial variation in expression levels between individual patients. Expression levels varied considerably depending on
the location of the primary tumor, with distinctly lower values in NEN originating from appendix and colon as compared to tumors from other intestinal origins. We also observed significantly
lower expression levels in MTS than in PT. SST2A expression declined depending on the malignancy of the tumor and there was a distinct association between SST2A expression and patient
outcome. Since CXCR4 presence was inversely correlated with SST2A expression especially in high-grade neuroendocrine carcinomas of the appendix or colon, this receptor may represent an
interesting new target structure, which should be validated in further studies. DATA AVAILABILITY The datasets used and/or analysed during the current study are available from the
corresponding author on reasonable request. REFERENCES * Furusato, B. & Rhim, J. S. CXCR4 and cancer. _Pathol. Internat._ 7, 497–505 (2010). Article Google Scholar * Zhao, H. _et al_.
CXCR4 over-expression and survival in cancer: A system review and meta-analysis. _Oncotarget._ 6, 5022–5040 (2015). PubMed Google Scholar * Corleto, V. D. _et al_. Somatostatin receptor
subtypes 2 and 5 are associated with better survival in well-differentiated endocrine carcinomas. _Neuroendocrinol._ 89, 223–230 (2009). Article CAS Google Scholar * Srirajaskanthan, R.,
Watkins, J., Marelli, L., Khan, K. & Caplin, M. E. Expression of somatostatin and dopamine 2 receptors in neuroendocrine tumours and the potential role for new biotherapies.
_Neuroendocrinol._ 89, 308–314 (2009). Article CAS Google Scholar * Zamora, V. _et al_. Immunohistochemical expression of somatostatin receptors in digestive endocrine tumours. _Dig. Liv.
Dis._ 42, 220–225 (2010). Article CAS Google Scholar * Okuwaki, K. _et al_. Clinicopathologic characteristics of pancreatic neuroendocrine tumors and relation of somatostatin receptor 2A
to outcomes. _Cancer._ 119, 4094–4102 (2013). Article CAS Google Scholar * Kaemmerer, D. _et al_. Inverse expression of somatostatin and CXCR4 chemokine receptors in
gastroenteropancreatic neuroendocrine neoplasms of different malignancy. _Oncotarget._ 6, 27566–27579 (2015a). PubMed PubMed Central Google Scholar * Mehta, S. _et al_. Somatostatin
receptor SSTR-2a expression is a stronger predictor for survival than Ki-67 in pancreatic neuroendocrine tumors. _Medicine._ 94, 1–6 (2015). Article Google Scholar * Qian, Z. R. _et al_.
Association between somatostatin receptor expression and clinical outcomes in neuroendocrine tumors. _Pancreas._ 45, 1386–1393 (2016). Article CAS Google Scholar * Song, K. B. _et al_.
Prognostic value of somatostatin receptor subtypes in pancreatic neuroendocrine tumors. _Pancreas._ 45, 187–192 (2016). Article CAS Google Scholar * Wada, H. _et al_. Expression of
somatostatin receptor type 2A and PTEN in neuroendocrine neoplasms is associated with tumor grade but not with site of origin. _Endocr. Pathol._ 27, 179–187 (2016). Article CAS Google
Scholar * Wang, Y. _et al_. Somatostatin receptor expression indicates improved prognosis in gastroenteropancreatic neuroendocrine neoplasm, and octreotide long-acting release is effective
and safe in Chinese patients with advanced gastroenteropancreatic neuroendocrine tumors. _Oncol. Lett._ 13, 1165–1174 (2017). Article CAS Google Scholar * Konukiewitz, B. _et al_.
Somatostatin receptor expression related to TP53 and RB1 alterations in pancreatic and extrapancreatic neuroendocrine neoplasms with a Ki67-index above 20%. _Mod. Pathol._ 30, 587–598
(2017). Article CAS Google Scholar * Deschamps, L. _et al_. The expression of the hypoxia markers CA9 and CXCR4 is correlated with survival in patients with neuroendocrine tumours of the
ileum. _Neuroendocrinol._ 95, 214–222 (2012). Article CAS Google Scholar * Kaemmerer, D. _et al_. Analysis of somatostatin receptor 2A immunohistochemistry, RT-qPCR, and _in vivo_ PET/CT
data in patients with pancreatic neuroendocrine neoplasm. _Pancreas._ 44, 648–654 (2015b). CAS PubMed Google Scholar * Circelli, L. _et al_. CXCR4/CXCL12/CXCR7 axis is functional in
neuroendocrine tumors and signals in mTOR. _Oncotarget._ 7, 18865–18875 (2016). Article Google Scholar * Brunner, P. _et al_. The prognostic and predictive value of
sstr2-immunohistochemistry and sstr2-targeted imaging in neuroendocrine tumors. _Eur. J. Nucl. Med. Imaging._ 44, 468–475 (2017). Article CAS Google Scholar * Yildiz, O. _et al_.
Gastroenteropancreatic neuroendocrine tumors: 10-year experience in a single center. _Med. Oncology._ 27, 1050–1056 (2010). Article Google Scholar * Fischer, T. _et al_. Reassessment of
sst2 somatostatin receptor expression in human normal and neoplastic tissues using the novel rabbit monoclonal antibody UMB-1. _J. Clin. Endocrinol. Metab._ 93, 4519–4524 (2008a). Article
CAS Google Scholar * Fischer, T., Nagel, F., Jacobs, S., Stumm, R. & Schulz, S. Reassessment of CXCR4 chemokine receptor expression in human normal and neoplastic tissues using the
novel rabbit monoclonal antibody UMB-2. _PLoS One._ 3, e4069 (2008b). Article ADS Google Scholar * Lupp, A. _et al_. Reassessment of sst5 somatostatin receptor expression in normal and
neoplastic human tissues using the novel rabbit monoclonal antibody UMB-4. _Neuroendocrinol._ 94, 255–264 (2011). Article CAS Google Scholar * Lupp, A. _et al_. Reassessment of sst3
somatostatin receptor expression in normal and neoplastic human tissues using the novel rabbit monoclonal antibody UMB-5. _Neuroendocrinol._ 96, 301–310 (2012). Article CAS Google Scholar
* Lupp, A., Nagel, F. & Schulz, S. Reevaluation of sst1 somatostatin receptor expression in human normal and neoplastic tissues using the novel rabbit monoclonal antibody UMB-7.
_Regul. Pept._ 183, 1–6 (2013). Article CAS Google Scholar * Lupp, A., Danz, M. & Müller, D. Morphology and cytochrome P450 isoforms expression in precision-cut rat liver slices.
_Toxicology._ 161, 53–66 (2001). Article CAS Google Scholar * Remmele, W. & Stegner, H. E. Recommendation for uniform definition of an immunoreactive score (IRS) for
immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. _Pathologe._ 8, 138–140 (1987). CAS PubMed Google Scholar * Van Gompel, J. J., Sippel, R. S., Warner, T.
F. & Chen, H. Gastrointestinal carcinoid tumors: Factors that predict outcome. _World J. Surg._ 28, 387–392 (2004). Article Google Scholar * Panzuto, F. _et al_. Prognostic factors and
survival in endocrine tumor patients: comparison between gastrointestinal and pancreatic localization. _Endocr. Rel. Cancer._ 12, 1083–1092 (2005). Article Google Scholar * Pape, U. F.
_et al_. Prognostic factors of long-term outcome in gastroenteropancreatic neuroendocrine tumours. _Endocr. Rel. Cancer._ 15, 1083–1097 (2008). Article Google Scholar * Ter-Minassian, M.
_et al_. Clinical presentation, recurrence, and survival in patients with neuroendocrine tumors: results from a prospective institutional database. _Endocr. Rel. Cancer._ 20, 187–196 (2013).
Article Google Scholar * Shanahan, M. A. _et al_. Chromogranin A predicts survival for resected pancreatic neuroendocrine tumors. _J. Surg. Res._ 201, 38–43 (2016). Article CAS Google
Scholar * Uppin, M. S. _et al_. Clinicopathologic study of neuroendocrine tumors of gastrointestinal tract: a single institutional experience. _J. Gastrointest. Oncol._ 8, 139–147 (2017).
Article Google Scholar * Papotti, M. _et al_. Expression of somatostatin receptor types 1-5 in 81 cases of gastrointestinal and pancreatic endocrine tumors. A correlative
immunohistochemical and reverse-transcriptase polymerase chain reaction analysis. _Virchows Arch._ 440, 461–475 (2002). Article CAS Google Scholar * Volante, M. _et al_. Somatostatin
receptor type 2 A immunohistochemistry in neuroendocrine tumors: a proposal of scoring system correlated with somatostatin receptor scintigraphy. _Modern Pathol._ 20, 1172–1182 (2007).
Article CAS Google Scholar * Sclafani, F. _et al_. Detection of somatostatin receptor subtypes 2 and 5 by somatostatin receptor scintigraphy and immunohistochemistry: clinical
implications in the diagnostic and therapeutic management of gastroenteropancreatic neuroendocrine tumors. _Tumori._ 97, 620–628 (2011). Article Google Scholar * Mizutani, G. _et al_.
Expression of somatostatin receptor (SSTR) subtypes (SSTR-1, 2A, 3, 4 and 5) in neuroendocrine tumors using real-time RT-PCR method and immunohistochemistry. _Acta Histochem. Cytochem._ 45,
167–176 (2012). Article CAS Google Scholar * Diakatou, E. _et al_. Somatostatin and dopamine receptor expression in neuroendocrine neoplasms: correlation of immunohistochemical findings
with somatostatin receptor scintigraphy visual scores. _Clin. Endocrinol._ 83, 420–428 (2015). Article CAS Google Scholar * Kaemmerer, D. _et al_. Molecular imaging with 68Ga-SSTR PET/CT
and correlation to immunohistochemistry of somatostatin receptors in neuroendocrine tumors. _Eur. J. Nucl. Med. Mol. Imaging._ 38, 1659–1668 (2011). Article CAS Google Scholar * Yao, J.
C. _et al_. Chromogranin A and neuron-specific enolase as prognostic markers in patients with advanced pNET treated with everolimus. _J. Clin. Endocrinol. Metab._ 96, 3741–3749 (2011).
Article CAS Google Scholar * Massironi, S. _et al_. Chromogranin A in diagnosing and monitoring patients with gastroenteropancreatic neuroendocrine neoplasms: a large series from a single
institution. _Neuroendocrinol._ 100, 240–249 (2014). Article CAS Google Scholar * Han, X. _et al_. The value of serum chromogranin A as a predictor of tumor burden, therapeutic response,
and nomogram-based survival in well – moderate non-functional pancreatic neuroendocrine tumors with liver metastases. _Eur. J. Gastroenterol. Hepatol._ 27, 527–535 (2015). Article Google
Scholar * Miederer, M. _et al_. Correlation of histopathological expression of somatostatin receptor 2 with standardised uptake values in 68Ga-DOTATOC PET/CT. _Eur. J. Nucl. Med. Mol.
Imaging._ 36, 48–52 (2009). Article CAS Google Scholar * Olsen, I. H. _et al_. 68Ga-DOTATOC PET and gene expression profile in patients with neuroendocrine carcinomas: strong correlation
between PET tracer uptake and gene expression of somatostatin receptor subtype 2. _Am. J. Nucl. Med. Mol. Imaging._ 6, 59–72 (2016). CAS PubMed PubMed Central Google Scholar * Körner,
M., Waser, B., Schonbrunn, A., Perren, A. & Reubi, J. C. Somatostatin receptor subtype 2A immunohistochemistry using a new monoclonal antibody selects tumors suitable for _in vivo_
somatostatin receptor targeting. _Am. J. Surg. Pathol._ 36, 242–252 (2012). Article Google Scholar * Öksüz, M. Ö. _et al_. Peptide receptor radionuclide therapy of neuroendocrine tumors
with (90)Y-DOTATOC: is treatment response predictable by pre-therapeutic uptake of (68)Ga-DOTATOC? _Diagn. Interv. Imaging._ 95, 289–300 (2014). Article Google Scholar * Kratochwil, C. _et
al_. SUV of [68Ga]DOTATOC-PET/CT predicts response probability of PRRT in neuroendocrine tumors. _Mol. Imaging Biol._ 17, 313–318 (2015). Article CAS Google Scholar * Venegas-Moreno, E.
_et al_. Association between dopamine and somatostatin receptor expression and pharmacological response to somatostatin analogues in acromegaly. _J. Cell. Mol. Med._ 22, 1640–1649 (2018).
Article CAS Google Scholar * Phan, G. Q. _et al_. Surgical experience with pancreatic and peripancreatic neuroendocrine tumors: review of 125 patients. _J. Gastrointest. Surg._ 2, 472–482
(1998). Article CAS Google Scholar * Wang, S. E. _et al_. Comparison of functional and nonfunctional neuroendocrine tumors in the pancreas and peripancreatic region. _Pancreas._ 40,
253–259 (2011). Article Google Scholar * Janot, M. S., Kersting, S., Herzog, T., Chromik, A. M. & Uhl, W. Prognosis and long-term survival after operation in patients with pancreatic
and peripancreatic neuroendocrine tumors of a single center. _J. Pancreas._ 17, 182–188 (2016). Google Scholar Download references ACKNOWLEDGEMENTS The Theranostic Research Center,
Zentralklinik Bad Berka, 99437 Bad Berka, Germany, provided funding for this research. AUTHOR INFORMATION Author notes * Rebekka Mai and Daniel Kaemmerer contributed equally. AUTHORS AND
AFFILIATIONS * Institute of Pharmacology and Toxicology, Jena University Hospital, Jena, Germany Rebekka Mai, Tina Träger, Elisa Neubauer, Stefan Schulz & Amelie Lupp * Department of
General and Visceral Surgery, Zentralklinik Bad Berka, Bad Berka, Germany Daniel Kaemmerer * Institute of Pathology and Cytology Bad Berka, Bad Berka, Germany Jörg Sänger * Center for
Molecular Radiotherapy and Molecular Imaging, Zentralklinik Bad Berka, Bad Berka, Germany Richard P. Baum Authors * Rebekka Mai View author publications You can also search for this author
inPubMed Google Scholar * Daniel Kaemmerer View author publications You can also search for this author inPubMed Google Scholar * Tina Träger View author publications You can also search for
this author inPubMed Google Scholar * Elisa Neubauer View author publications You can also search for this author inPubMed Google Scholar * Jörg Sänger View author publications You can also
search for this author inPubMed Google Scholar * Richard P. Baum View author publications You can also search for this author inPubMed Google Scholar * Stefan Schulz View author
publications You can also search for this author inPubMed Google Scholar * Amelie Lupp View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS
Conceived and designed the experiments: D.K., A.L. Provided the tumor samples: J.S. Provided the antibodies: S.S. Provided the clinical data: D.K., R.P.B. Performed the experiments: R.M.,
T.T., E.N., A.L. Analyzed the data: R.M., R.P.B., A.L. Wrote the paper: A.L. Each of the authors has approved the manuscript and acknowledges that he or she participated sufficiently in the
work to take public responsibility for its content. CORRESPONDING AUTHOR Correspondence to Amelie Lupp. ETHICS DECLARATIONS COMPETING INTERESTS Daniel Kaemmerer received support for
travelling to meetings by the companies IPSEN and PFIZER. All other authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the
research reported. ADDITIONAL INFORMATION PUBLISHER’S NOTE: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which permits
use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the
Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated
otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds
the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/. Reprints and
permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Mai, R., Kaemmerer, D., Träger, T. _et al._ Different somatostatin and CXCR4 chemokine receptor expression in gastroenteropancreatic
neuroendocrine neoplasms depending on their origin. _Sci Rep_ 9, 4339 (2019). https://doi.org/10.1038/s41598-019-39607-2 Download citation * Received: 16 August 2018 * Accepted: 28 January
2019 * Published: 13 March 2019 * DOI: https://doi.org/10.1038/s41598-019-39607-2 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable
link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative