Play all audios:
ABSTRACT This study was aimed to compare serial long-term postoperative changes in quality-of-life (QoL) between photoselective-vaporization (PVP) using 120W-High-Performance-System and
holmium-laser-enucleation (HoLEP) in benign-prostatic-hyperplasia (BPH) patients and to identify factors influencing the QoL improvement at the short-term, mid-term and long-term follow-up
visits after surgery. We analyzed 1,193 patients with a baseline QoL-index ≥2 who underwent PVP (n = 439) or HoLEP (n = 754). Surgical outcomes were serially compared between the two groups
at up to 60-months using the International-Prostatic-Symptom-Score (I-PSS), uroflowmetry, and serum PSA. We used logistic regression analysis to identify predictors of QoL improvement (a
reduction in the QoL-index ≥50% compared with baseline) at the short-term (12-months), mid-term (36-months), and long term (60-months) follow-up after surgery. In both groups, the QoL-index
was decreased throughout the entire follow-up period compared with that at baseline. There were no significant differences in postoperative changes from the baseline QoL-index between the
two groups during the 48-month follow-up, except at 60-months. The degree of improvement in QoL at 60-months after HoLEP was greater than that after PVP. A lower baseline
storage-symptom-subscore and a higher bladder-outlet-obstruction-index (BOOI) were independent factors influencing QoL improvement at the short-term. No independent factor influences QoL
improvement at the mid- or long-term. SIMILAR CONTENT BEING VIEWED BY OTHERS SEXUAL AND EJACULATORY FUNCTION AFTER HOLMIUM LASER ENUCLEATION OF THE PROSTATE AND BIPOLAR TRANSURETHRAL
ENUCLEATION OF THE PROSTATE: A SINGLE-CENTER EXPERIENCE Article 20 October 2020 RELATIONSHIPS BETWEEN HOLMIUM LASER ENUCLEATION OF THE PROSTATE AND PROSTATE CANCER Article 23 November 2022
SHORT TERM RESULTS AFTER MINIMALLY INVASIVE TREATMENTS FOR BENIGN PROSTATIC ENLARGEMENT: THE FIRST RANDOMIZED TRIAL COMPARING TRANSPERINEAL LASER ABLATION AND WATER VAPOR ABLATION Article 25
April 2025 INTRODUCTION Lower urinary tract symptoms (LUTS) caused by benign prostatic hyperplasia (BPH) is known to be a highly prevalent disease with increasing age1,2,3, and it is
directly and negatively related to the quality of life (QoL)2,4. As expectations for QoL are increasing with increased life expectancy, many elderly men with LUTS become less tolerant5 and
complain about LUTS, leading to poor QoL, although LUTS due to BPH is not life threatening. Thus, one of the aims of treatment for BPH patients is improving QoL through improving LUTS6, and,
to improve LUTS and QoL in men with severe LUTS, surgical treatment would be useful5. For decades, standard treatment for BPH was transurethral prostatectomy (TURP)3,7,8. Recently, as
alternatives for TURP, laser surgeries such as photoselective vaporization of the prostate (PVP) and holmium laser enucleation of the prostate (HoLEP) have been increasingly performed9,
because of fewer perioperative complications, which are related to perioperative QoL10. Specifically, in several studies, PVP and HoLEP were reported to have, at least, noninferior efficacy,
less bleeding, and less catheter duration than TURP11. Thus, PVP was recommended in patients with a high cardiovascular risk and high bleeding risk12; additionally, HoLEP has an advantage
regarding hemostasis13. As less complications would be expected to lead to better QoL as mentioned above10, PVP and HoLEP could be the good option to LUTS patient who pursuit QoL. To the
best of our knowledge, few studies have directly compared postoperative treatment outcomes between PVP and HoLEP, focusing on improvement in QoL during a serial long-term follow-up period,
although a few short-term follow-up studies showed no significant differences in the postoperative improvement of QoL during a one-year follow-up after surgery14,15. Additionally, few
studies have investigated which factors could influence postoperative improvements in QoL after the two laser surgeries. Therefore, the aim of this study was to compare serial long-term
postoperative changes in QoL between PVP using a 120-W GreenLight high-performance system (HPS) and HoLEP in patients with BPH and to determine the factors influencing the improvement of QoL
at the short-term, mid-term, and long-term follow-up visits after surgery using a serial long-term follow-up database. RESULTS BASELINE CHARACTERISTICS In comparing the baseline
characteristics between the PVP and HoLEP groups, the PVP group had a higher level of serum PSA, a smaller prostate volume, a higher voiding symptom score (VSS), a higher storage symptom
score (SSS), a higher total International Prostate Symptom Score (I-PSS), a longer operation time, and greater energy applied during the surgeries than the HoLEP group (Table 1). However,
the baseline QoL index was not different between the groups. Regarding the baseline urodynamic data, the HoLEP group showed a smaller postvoid residual urine volume (PVR), a smaller maximum
cystometric capacity (MCC), a higher bladder outlet obstruction index (BOOI), a higher bladder contractility index (BCI), and a higher percentage of patients with involuntary detrusor
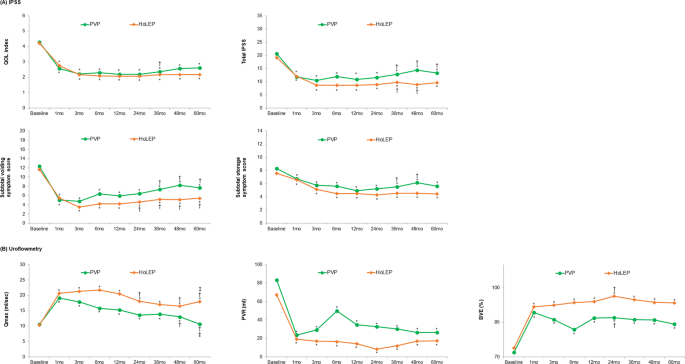
contraction (IDC) than the PVP group (Table 1). SERIAL POSTOPERATIVE OUTCOMES AFTER PVP OR HOLEP In both the PVP and HoLEP groups, the value of the QoL index at each follow-up visit was
significantly decreased during the entire follow-up period after surgery compared with that at the baseline (Fig. 1). Additionally, according to the repeated measures analysis of variance
(ANOVA) test to adjust for the effect of time on the QoL outcomes, no significant differences were found in the change of the QoL index over time between the PVP and HoLEP groups during the
60-month follow-up period (Supplementary Fig. S2). The improvement in all outcomes parameters, including total I-PSS, VSS, SSS, the maximum flow rate (_Q_max), PVR, and bladder voiding
efficiency (BVE), was maintained during the entire follow-up period after PVP or HoLEP, except for _Q_max at 60 months after PVP. However, the values of VSS and SSS starting from 36 months
after the PVP were increased compared with those at 12 months after surgery, although their decrease was sustained up to 60 months after surgery compared with that at baseline. Meanwhile,
the values of VSS starting from 24 months after the HoLEP were increased compared with those at 12 months after surgery, whereas those of SSS at 24, 36, 48 and 60 months after surgery were
not different from 12 months postoperatively. The _Q_max values in both the PVP and HoLEP groups were deteriorated starting from 24 months compared with those at 12 months after surgery.
However, the increase in the _Q_max value at all follow visits after the HoLEP was maintained up to 60 months compared with that at baseline, whereas the _Q_max value at 60 months after the
PVP was decreased to the baseline level. The incidence of transient urinary incontinence after HoLEP was higher than that after PVP (Table 2). Repeated BPH surgeries because of the regrowth
of prostatic adenoma were performed for 12 patients in the PVP group but for none in the HoLEP group. COMPARISON OF THE POSTOPERATIVE CHANGES IN OUTCOME PARAMETERS BETWEEN PVP AND HOLEP TO
THAT AT THE BASELINE In terms of postoperative changes from the baseline in the QoL index, no significant differences were found between the groups during the 48-month follow-up period after
surgery. However, the degree of reduction in the QoL index at 60 months after HoLEP was greater than that after PVP (Fig. 2). The percentages of patients with QoL improvement were 54.0%,
52.2%, and 43.1% at 1-, 3- and 5-years after PVP, and 57.7%, 53.7%, and 55.3% at 1-, 3- and 5-years after HoLEP, respectively (Supplementary Table S1). The degree of reduction in the total
I-PSS and VSS during the entire follow-up period after HoLEP was greater than that after PVP, except for that at one month and 24 months after the surgeries (Fig. 2). Additionally, the
degree of increase in _Q_max during the entire follow-up period after HoLEP was greater than that after PVP, except for that at one month and 36 months after the surgeries (Fig. 2). However,
no significant differences were found in the postoperative changes in the other outcome parameters (SSS, PVR, and BVE) compared with that at baseline between the two groups throughout the
entire follow-up period after surgery. The degree of decrease in the serum PSA level at each follow-up visit after HoLEP was generally greater than that after PVP. INFLUENTIAL FACTOR OF QOL
IMPROVEMENT AFTER PVP OR HOLEP According to logistic regression (LR) analyses, univariate analysis showed that the serum PSA level, preoperative prostate volume, baseline SSS, BCI, BOOI on
baseline urodynamic study (UDS), operation time, and energy applied during surgery were associated with QoL improvement at one year after surgery. Multivariate analysis revealed that lower
baseline SSS and higher BOOI were independent factors influencing QoL improvement at the short-term follow-up visit after surgery (Table 3). In terms of influential factors of QoL
improvement at the mid-term follow-up visit, the univariate model showed that the preoperative prostate volume, BOOI on baseline UDS, operation time, and energy applied during surgery were
associated with QoL improvement at three years after surgery. However, on multivariate analysis, no independent factor influenced QoL improvement at that time (Table 3). Regarding
influential factors of QoL improvement at the long-term follow-up visit, univariate analysis revealed no factor influencing QoL improvement at five years after surgery. The surgical methods
were not associated with QoL improvement at any time point of follow-up after surgery (Table 3). DISCUSSION Because LUTS strongly influences QoL negatively2,4, one of the goals for the
treatment of BPH was focused on improving QoL16. Laser surgery for BPH has been expected to be alternatives to the gold standard of BPH surgery (TURP or open prostatectomy) because, compared
with TURP, it showed comparable efficacy and lower postoperative morbidity as mentioned above11,17. Specifically, Xue _et al_. reported that PVP provided equivalent efficacy and fewer
bleeding complications for 3 years after surgery, compared with TURP18. HoLEP, an enucleation surgery for BPH, was reported to have similar efficacy and lower perioperative complications
with a significant level of evidence, than TURP8. However, there has been a scarcity of studies mainly focusing on QoL improvement after laser prostatectomy. Because the treatment outcomes
of BPH surgery greatly affect patients’ QoL, this study may extend the current knowledge regarding them. The results of our study are summarized as follows: * (1) Postoperative improvement
of QoL was maintained up to the long-term follow-up period after PVP or HoLEP. * (2) No significant differences were found between the two groups in postoperative changes from baseline of
the QoL index during the 48-month follow-up period after surgery. However, the degree of improvement in QoL at 60 months after HoLEP was greater than that after PVP. * (3) Lower baseline SSS
and higher BOOI were independent factors influencing QoL improvement at the short-term follow-up visit after surgery. However, because the follow-up duration was longer, no independent
factor influenced QoL improvement at the mid- and long-term follow-up visits after surgery. Our study has shown that the postoperative improvement of QoL was maintained up to the long-term
follow-up period, irrespective of the type of laser surgery. In agreement with our results, Xue _et al_. reported that the postoperative improvement of QoL was sustained up to 36 months
after TURP or PVP-120 W-HPS18. Additionally, Gilling _et al_. compared the surgical outcomes at 1, 3, 6, 12, 24 and 92 months between TURP and HoLEP19. According to their results, the
postoperative improvement of QoL was maintained up to 92 months after TURP and HoLEP, without a difference between the two surgeries19. Meanwhile, although laser surgery is expected to have
a positive effect on the postoperative improvement of QoL in men with BPH, few studies have focused on the comparative analysis of serial long-term treatment outcomes for QoL between PVP and
HoLEP. Previously, a minority of studies showed no difference in the postoperative improvement of QoL at one year after surgery between PVP using 120 W HPS and HoLEP14,15. Interestingly,
our study with long-term follow-up data showed that the degree of improvement in the QoL index at 60-month follow-up visits after HoLEP might be superior to that after PVP, perhaps in part
because of a difference in the long-term durability of surgical outcomes. This result could be supported by our finding that the degree of improvement in voiding symptoms, peak flow rate or
reduction in the serum PSA level at the long-term follow-up visits after HoLEP was higher than that after PVP. In accordance with these findings, recent literature by Hermann _et al_. noted
that transurethral endoscopic enucleation of the prostate, such as HoLEP, offer some advantages in terms of morbidity8,13. However, further long-term follow-up studies comparing PVP using
the 180 W XPS laser and HoLEP are necessary to draw a solid conclusion because PVP using the 180 W XPS laser has recently been performed in men with BPH. Interestingly, according to our
data, the degree of improvement in voiding symptoms during the early postoperative period (1 to 3 months) after PVP or HoLEP was much greater than that in storage symptoms. Thus, storage
symptoms appear to improve gradually with time after surgery, whereas voiding symptoms do dramatically from the immediate postoperative period after surgery. This may be attributed to an
irritative effect of laser vaporization despite enucleation during laser prostatectomy. Thus, laser energy applied during laser prostatectomy might be beneficial with respect to hemostasis,
but some patients could pay the price of postoperative storage or irritative symptoms in the early postoperative period. The irritative effect may have impacts on the surgical outcome for
storage symptoms in the early postoperative period. In accordance with this, Cindolo _et al_. showed that transient storage symptoms were developed more frequently after GreenLight
enucleation of the prostate than after standard PVP or anatomic PVP20. They suggested that this might be due to microinjury of capsules and per-capsule innervation caused by more coagulation
in the capsular bleeding spot in GreenLight enucleation of the prostate20. A factor to be considered when evaluating the surgical outcomes of PVP or HoLEP is the surgeon’s expertise.
Particularly regarding the learning curve of HoLEP, some literature has shown that HoLEP has a steep learning curve with a stationary state at 20–50 cases21,22. Accordingly, when the
learning curve for the efficiency of HoLEP was assessed by enucleation efficiency (a ratio of retrieved tissue weight/enucleation time) in our study, the enucleation efficiency appeared to
be stationary after approximately 50 cases (Supplementary Fig. S1B). According to a recent study by Castellan _et al_. that analyzed a learning curve of PVP using the 180 W XPS laser,
surgeons with greater experience in endoscopic procedure showed a lower rate of early complications and greater evolution in lasing time/operation time ratio than those with lesser
experience23. However, there was no significant difference in the functional outcomes at 6 months after surgery between the groups23. In the present study, when the learning curve for the
efficiency of PVP was assessed by the ratio of the removed prostate volume/operation time, the PVP efficiency seemed to be stationary even in the first case. Furthermore, the PVP efficiency
was further evolved after approximately 150 cases. The cause might be that the surgeon (HS) in our study had sufficient experience in endoscopic surgery for BPH. However, it is difficult to
directly compare the studies because of differences in the baseline characteristics and study populations, as well as in definitions of learning curve. To our knowledge, this is the first
study that reported the factors influencing the postoperative improvement of QoL serially at the short-term, mid-term, and long-term follow-up visits after PVP or HoLEP. Our LR analyses
showed that a lower baseline SSS and a higher BOOI were independent factors influencing postoperative QoL improvement at the short-term follow-up visit after PVP or HoLEP. Given that BPH
surgeries such as PVP and HoLEP have been designed to relieve BOO, it may be reasonable to assume that patients with a higher BOOI have a higher probability of improvement in QoL after
surgery. In accordance with our result, Ryoo _et al_. showed that a BOOI greater than 40 was a predictor of treatment success, including QoL at six months after HoLEP24. Additionally, the
patients with less severe storage symptoms before surgery appear to have a higher possibility of postoperative improvement in QoL, perhaps because, as our data showed, the lower baseline SSS
was significantly correlated with a lower SSS and a lower QoL index at one year after PVP or HoLEP (Spearman’s correlation coefficient = 0.390 and 0.253, respectively). Interestingly, based
on univariate analysis, several factors, including a higher BOOI and preoperative prostate volume, were associated with postoperative QoL improvement at the mid-term follow-up visit, no
independent factor of QoL improvement was found on multivariate analysis. Furthermore, no influential factor of QoL improvement was found at the long-term follow-up visit, even on univariate
analysis. Thus, postoperative QoL improvement at the short-term follow-up period after PVP or HoLEP appears to be maintained up to five years, without any specific factor influencing its
improvement at the mid-term or long-term follow-up visit. There are a few limitations in our study. First, because our study was retrospective, there were differences in a few baseline
parameters between the two groups. Second, we used PVP using 120 W-HPS; however, in 2010, PVP using 180 W-XPS was introduced. In the future, long-term follow-up studies comparing PVP using
the 180 W XPS laser and HoLEP are necessary to validate our result, although the long-term follow-up data of PVP using 180 W-GreenLight XPS might still be limited. Nevertheless, our data
have some clinical implications to understand the outcomes of QoL-related LUTS after laser prostatectomy, such as PVP or HoLEP. Our results may help effectively counsel patients about
expectations for two representative laser prostatectomies or surgical outcomes for QoL related to LUTS. Additionally, our results may be used to counsel patients on which ones can benefit
the most from PVP or HoLEP in terms of QoL-related LUTS, particularly at the short-term follow-up period after surgery. In conclusion, our data confirm that both PVP and HoLEP have durable
efficacy in QoL improvement throughout the five-year follow-up period. HoLEP might provide more improvement in QoL at the long-term follow-up point than PVP. A lower baseline SSS and a
higher BOOI appear to independently influence QoL improvement at the short-term follow-up visit after PVP or HoLEP. When the follow-up duration is longer, no factor appears to influence QoL
improvement independently at the mid- and long-term follow-up visits. Subsequent prospectively controlled comparative studies with a larger study population and a long-term follow-up on PVP
using 180 W GreenLight XPS and HoLEP would be needed to validate our findings. MATERIALS AND METHODS STUDY POPULATION, DATA AND DESIGN This study was approved by the Institutional Review
Board at both Seoul National University and Seoul Metropolitan Government Seoul National University Boramae Medical Center. All methods in this study were carried out in accordance with
relevant guidelines and regulations. The need for written informed consent was waived because of the retrospective nature of this study. We retrospectively reviewed the data of 1,569
patients who had undergone PVP-120 W-HPS (n = 564) or HoLEP (n = 1,005) because their LUTS/BPH was unresponsive to medications from January 2008 to March 2014 at our institution. We excluded
320 patients with previously diagnosed urethral stricture, cancer of the bladder or prostate or urethra, history of other urologic surgeries, or incomplete data. Among the remaining 1,249
patients, 1,193 patients (PVP group, n = 439; HoLEP group, n = 754) with a baseline QoL of the I-PSS of at least 2 before surgery were included in this study. Before the surgeries, all
patients received preoperative evaluations for LUTS secondary to BPH, including medical history, physical examinations, the I-PSS, urinalysis, serum PSA, transrectal ultrasound for prostate,
and a multichannel UDS. A surgical method, either PVP or HoLEP, was chosen based on the surgeon’s preference. PVP was performed by a single surgeon (HS) as described in a previous study25.
Briefly, PVP was performed using the planned vaporization-resection technique, with a 120 W GreenLight HPS laser at a setting of 80 W for vaporization-resection and 100 W for vaporization.
HoLEP was performed by one of two surgeons (JSP or SJO) in the usual manner as previously mentioned26. Briefly, enucleation was performed mainly using three-lobe techniques with a 26 Fr
resectoscope, a 550-μm laser fiber, or an 80-W holmium:YAG laser at a setting of 2 J 50 Hz or 2 J 40 Hz. Morcellation of the enucleated prostatic adenoma was performed with a morcellator.
The patients received follow-up visits serially at 1, 3, 6, 12, 24, 36, 48 and 60 months after surgery. At each follow-up visit, the patients were evaluated for the I-PSS, serum PSA, and
uroflowmetry. We defined ‘QoL improvement’ as a reduction of 50% or more in the QoL index at each follow-up visit compared with that at the baseline to investigate patients with a definite
effect after surgery to confirm strong factors leading to favorable outcomes. Bladder voiding efficiency (BVE) was equated as (voided volume) × 100/(voided volume + PVR). STATISTICAL
ANALYSIS To compare the preoperative characteristics and surgical outcomes between PVP and HoLEP, we used independent t-test and chi-squared or Fisher’s exact test. For comparisons between
baseline variables and postoperative outcome parameters, we used paired t-test. Additionally, the repeated-measures ANOVA test was performed to adjust for the impact of time on the QoL
outcomes. To identify the factors influencing the ‘QoL improvement’ at the short-term (one year after surgery), mid-term (three years after surgery), and long-term (five years after
surgery), we applied LR analyses. Variables with p < 0.05 in the univariate LR were included in multiple LR. p < 0.05 was considered as statistically significant in all analyses.
Statistical analyses were performed using IBM SPSS version 21.0. DATA AVAILABILITY The analyzed data sets of this study can be reasonably requested from the corresponding author. CHANGE
HISTORY * _ 08 NOVEMBER 2019 An amendment to this paper has been published and can be accessed via a link at the top of the paper. _ REFERENCES * Berry, S. J., Coffey, D. S., Walsh, P. C.
& Ewing, L. L. The development of human benign prostatic hyperplasia with age. _J Urol_ 132, 474–479 (1984). Article CAS Google Scholar * Seki, N. _et al_. Association among the
symptoms, quality of life and urodynamic parameters in patients with improved lower urinary tract symptoms following a transurethral resection of the prostate. _Neurourol Urodyn_ 27,
222–225, https://doi.org/10.1002/nau.20466 (2008). Article PubMed Google Scholar * Cornu, J. N. Bipolar, Monopolar, Photovaporization of the Prostate, or Holmium Laser Enucleation of the
Prostate: How to Choose What’s Best? _Urol Clin North Am_ 43, 377–384, https://doi.org/10.1016/j.ucl.2016.04.006 (2016). Article PubMed Google Scholar * Fwu, C. W. _et al_. Long-term
effects of doxazosin, finasteride and combination therapy on quality of life in men with benign prostatic hyperplasia. _J Urol_ 190, 187–193, https://doi.org/10.1016/j.juro.2013.01.061
(2013). Article CAS PubMed Google Scholar * Garraway, W. M. & Kirby, R. S. Benign prostatic hyperplasia: effects on quality of life and impact on treatment decisions. _Urology_ 44,
629–636 (1994). Article CAS Google Scholar * DerSarkissian, M. _et al_. Comparing Clinical and Economic Outcomes Associated with Early Initiation of Combination Therapy of an Alpha
Blocker and Dutasteride or Finasteride in Men with Benign Prostatic Hyperplasia in the United States. _J Manag Care Spec Pharm_ 22, 1204–1214, https://doi.org/10.18553/jmcp.2016.22.10.1204
(2016). Article PubMed Google Scholar * Djavan, B. _et al_. Benign prostatic hyperplasia: current clinical practice. _Prim Care_ 37, 583–597, ix, https://doi.org/10.1016/j.pop.2010.04.004
(2010). Article PubMed Google Scholar * Naspro, R. _et al_. From “gold standard” resection to reproducible “future standard” endoscopic enucleation of the prostate: what we know about
anatomical enucleation. _Minerva Urol Nefrol_ 69, 446–458, https://doi.org/10.23736/S0393-2249.17.02834-X (2017). Article PubMed Google Scholar * Hueber, P. A. & Zorn, K. C. Canadian
trend in surgical management of benign prostatic hyperplasia and laser therapy from 2007-2008 to 2011-2012. _Can Urol Assoc J_ 7, E582–586, https://doi.org/10.5489/cuaj.203 (2013). Article
PubMed PubMed Central Google Scholar * Archer, S. _et al_. Surgery, Complications, and Quality of Life: A Longitudinal Cohort Study Exploring the Role of Psychosocial Factors. _Ann Surg_,
https://doi.org/10.1097/SLA.0000000000002745 (2018). Article Google Scholar * Cornu, J. N. _et al_. A Systematic Review and Meta-analysis of Functional Outcomes and Complications
Following Transurethral Procedures for Lower Urinary Tract Symptoms Resulting from Benign Prostatic Obstruction: An Update. _Eur Urol_ 67, 1066–1096,
https://doi.org/10.1016/j.eururo.2014.06.017 (2015). Article PubMed Google Scholar * Brassetti, A. _et al_. Green light vaporization of the prostate: is it an adult technique? _Minerva
Urol Nefrol_ 69, 109–118, https://doi.org/10.23736/S0393-2249.16.02791-0 (2017). Article PubMed Google Scholar * Herrmann, T. R. Enucleation is enucleation is enucleation is enucleation.
_World J Urol_ 34, 1353–1355, https://doi.org/10.1007/s00345-016-1922-3 (2016). Article PubMed Google Scholar * Elzayat, E. A., Al-Mandil, M. S., Khalaf, I. & Elhilali, M. M. Holmium
laser ablation of the prostate versus photoselective vaporization of prostate 60 cc or less: short-term results of a prospective randomized trial. _J Urol_ 182, 133–138,
https://doi.org/10.1016/j.juro.2009.02.117 (2009). Article PubMed Google Scholar * Elmansy, H. _et al_. Holmium laser enucleation versus photoselective vaporization for prostatic adenoma
greater than 60 ml: preliminary results of a prospective, randomized clinical trial. _J Urol_ 188, 216–221, https://doi.org/10.1016/j.juro.2012.02.2576 (2012). Article PubMed Google
Scholar * Madersbacher, S. _et al_. EAU 2004 guidelines on assessment, therapy and follow-up of men with lower urinary tract symptoms suggestive of benign prostatic obstruction (BPH
guidelines). _Eur Urol_ 46, 547–554, https://doi.org/10.1016/j.eururo.2004.07.016 (2004). Article PubMed Google Scholar * Zang, Y. C. _et al_. Photoselective vaporization of the prostate
with GreenLight 120-W laser versus transurethral resection of the prostate for benign prostatic hyperplasia: a systematic review with meta-analysis of randomized controlled trials. _Lasers
Med Sci_ 31, 235–240, https://doi.org/10.1007/s10103-015-1843-1 (2016). Article PubMed Google Scholar * Xue, B. _et al_. GreenLight HPS 120-W laser vaporization versus transurethral
resection of the prostate for treatment of benign prostatic hyperplasia: a prospective randomized trial. _J Xray Sci Technol_ 21, 125–132, https://doi.org/10.3233/XST-130359 (2013). Article
PubMed Google Scholar * Gilling, P. J. _et al_. Long-term results of a randomized trial comparing holmium laser enucleation of the prostate and transurethral resection of the prostate:
results at 7 years. _BJU Int_ 109, 408–411, https://doi.org/10.1111/j.1464-410X.2011.10359.x (2012). Article PubMed Google Scholar * Cindolo, L., Ruggera, L., Destefanis, P., Dadone, C.
& Ferrari, G. Vaporize, anatomically vaporize or enucleate the prostate? The flexible use of the GreenLight laser. _Int Urol Nephrol_ 49, 405–411,
https://doi.org/10.1007/s11255-016-1494-6 (2017). Article PubMed Google Scholar * Robert, G. _et al_. Multicentre prospective evaluation of the learning curve of holmium laser enucleation
of the prostate (HoLEP). _BJU Int_ 117, 495–499, https://doi.org/10.1111/bju.13124 (2016). Article PubMed Google Scholar * Kampantais, S. _et al_. Assessing the Learning Curve of Holmium
Laser Enucleation of Prostate (HoLEP). A Systematic Review. _Urology_ 120, 9–22, https://doi.org/10.1016/j.urology.2018.06.012 (2018). Article PubMed Google Scholar * Castellan, P. _et
al_. The Surgical Experience Influences the Safety and Efficacy of Photovaporization of Prostate with 180-W XPS GreenLight Laser: Comparison Between Novices vs Expert Surgeons Learning
Curves. _J Endourol_ 32, 1071–1077, https://doi.org/10.1089/end.2018.0437 (2018). Article PubMed Google Scholar * Ryoo, H. S. _et al_. Efficacy of Holmium Laser Enucleation of the
Prostate Based on Patient Preoperative Characteristics. _Int Neurourol J_ 19, 278–285, https://doi.org/10.5213/inj.2015.19.4.278 (2015). Article PubMed PubMed Central Google Scholar *
Yoo, S. _et al_. A novel vaporization-enucleation technique for benign prostate hyperplasia using 120-W HPS GreenLight laser: Seoul technique II in comparison with vaporization and
previously reported modified vaporization-resection technique. _World J Urol_ 35, 1923–1931, https://doi.org/10.1007/s00345-017-2091-8 (2017). Article PubMed Google Scholar * Kim, M.,
Lee, H. E. & Oh, S. J. Technical aspects of holmium laser enucleation of the prostate for benign prostatic hyperplasia. _Korean J Urol_ 54, 570–579,
https://doi.org/10.4111/kju.2013.54.9.570 (2013). Article PubMed PubMed Central Google Scholar Download references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of Urology,
Seoul National University College of Medicine, SMG-SNU Boramae Medical Center, Seoul, 07061, Republic of Korea Sangjun Yoo, Juhyun Park, Sung Yong Cho, Hyeon Jeong, Hwancheol Son & Min
Chul Cho * Department of Urology, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, 03080, Republic of Korea Inyoung Sun, Seung-June Oh &
Jae-Seung Paick Authors * Inyoung Sun View author publications You can also search for this author inPubMed Google Scholar * Sangjun Yoo View author publications You can also search for this
author inPubMed Google Scholar * Juhyun Park View author publications You can also search for this author inPubMed Google Scholar * Sung Yong Cho View author publications You can also
search for this author inPubMed Google Scholar * Hyeon Jeong View author publications You can also search for this author inPubMed Google Scholar * Hwancheol Son View author publications You
can also search for this author inPubMed Google Scholar * Seung-June Oh View author publications You can also search for this author inPubMed Google Scholar * Jae-Seung Paick View author
publications You can also search for this author inPubMed Google Scholar * Min Chul Cho View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS
I.S. carried out substantial contributions to the conception/design, data acquisition, data analysis, interpretations, drafting of the manuscript and statistical analysis. S.Y. carried out
substantial contributions to the conception/design, data acquisition, data analysis, interpretations and statistical analysis. J.P., S.Y.C., H.J. carried out data analysis and data
interpretation. H.S., S.J.O. and J.S.P. carried out substantial contributions to the data acquisition, data interpretation and drafting of the manuscript. M.C.C. carried out substantial
contributions to the conception/design, data interpretation, drafting of the manuscript, supervision and final approval of the version to be published. All authors read and approved the
final manuscript. CORRESPONDING AUTHOR Correspondence to Min Chul Cho. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER’S
NOTE: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION RIGHTS AND
PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any
medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The
images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not
included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly
from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Sun, I., Yoo, S.,
Park, J. _et al._ Quality of life after photo-selective vaporization and holmium-laser enucleation of the prostate: 5-year outcomes. _Sci Rep_ 9, 8261 (2019).
https://doi.org/10.1038/s41598-019-44686-2 Download citation * Received: 15 February 2019 * Accepted: 22 May 2019 * Published: 04 June 2019 * DOI: https://doi.org/10.1038/s41598-019-44686-2
SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to
clipboard Provided by the Springer Nature SharedIt content-sharing initiative