Play all audios:
ABSTRACT In China, Henan Province is a region with a high HIV burden. Furthermore, drug resistance (DR) among people living with HIV/AIDS (PLWHA) on antiretroviral therapy (ART) is becoming
a critical barrier to achieving viral suppression. Monitoring DR in PLWHA with detectable viremia after ART is crucial, especially given the widespread use of NNRTI and NRTI, which have
historically been the backbone of China’s national ART program due to affordability and availability. In this study, plasma samples from PLWHA with viral load (VL) ≥ 40 copies/mL after ≥ 6
months of ART from January 2023 to December 2023 were collected for genotypic DR testing. Of 804 individuals with detectable viremia, a total of 14 HIV-1 subtypes were detected. The top five
subtypes were B (55.97%, 450/804), CRF01_AE (22.14%, 178/804), CRF07_BC (15.42%, 124/804), CFR55_01B (3.36%, 27/804), and CRF08_BC (1.00%, 8/804). DR analysis revealed a prevalence of
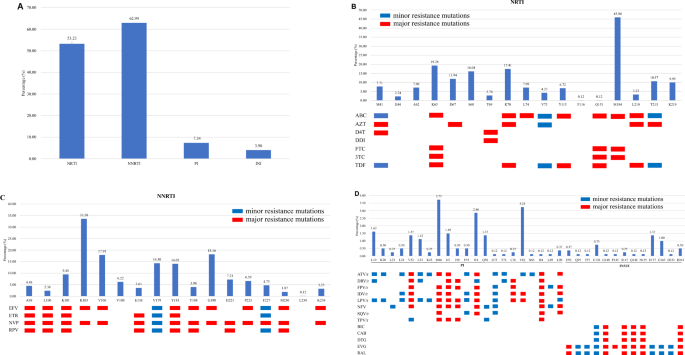
67.79% (545/804). The resistance rates for non-nucleoside reverse transcriptase inhibitors (NNRTIs), nucleoside reverse transcriptase inhibitors (NRTIs), protease inhibitors (PIs), and
integrase strand transfer inhibitors (INSTIs) were 62.94% (506/804), 53.23% (428/804), 7.34% (59/804), and 3.98% (32/804), respectively. The prevalence of DR among PLWHA below and ≥ 200
copies/mL were 40.63% (13/32) and 68.91% (532/772), respectively. Multivariate regression analysis showed that age < 29 years and 40–49 years, baseline CD4 count < 500 cells/µL,
current VL of 103–105 copies/mL, and initial ART regimen of NRTIs + NNRTIs were closely associated with the occurrence of DR. These findings highlight the urgent need for expanded access to
drug resistance testing and the adoption of WHO-recommended regimens, such as dolutegravir (DTG), to mitigate the growing threat of DR. Our results suggest that drug resistance testing
should be applied to all PLWHA with detectable viremia, and treatment strategies should be optimized to align with global guidelines. SIMILAR CONTENT BEING VIEWED BY OTHERS CHARACTERISTICS
OF DRUG RESISTANCE MUTATIONS IN ART-EXPERIENCED HIV-1 PATIENTS WITH LOW-LEVEL VIREMIA IN ZHENGZHOU CITY, CHINA Article Open access 09 May 2024 HIV-1 SUPPRESSION AND RARE DOLUTEGRAVIR
RESISTANCE IN ANTIRETROVIRAL-EXPERIENCED PEOPLE WITH HIV IN LIBERIA Article Open access 09 May 2025 HIV-1 DIVERSITY AND PRE-TREATMENT DRUG RESISTANCE IN THE ERA OF INTEGRASE INHIBITOR AMONG
NEWLY DIAGNOSED ART-NAÏVE ADULT PATIENTS IN LUANDA, ANGOLA Article Open access 10 July 2024 Since China launched antiretroviral therapy (ART) in 2003, the viral load (VL) of most human
immunodeficiency virus type 1 (HIV-1) infected individuals can be effectively controlled, greatly prolonging the life expectancy of people living with HIV/AIDS (PLWHA)1. However, widespread
ART inevitably leads to the emergence of drug resistance (DR) due to multiple factors, such as low genetic barrier of non-nucleoside reverse transcriptase inhibitors (NNRTIs) and nucleoside
reverse transcriptase inhibitors (NRTIs) and poor adherence2. The National Free Antiretroviral Treatment Program initially adopted NNRTIs and NRTIs as the main drugs in the standardized
regimens due to their affordability and availability, which subsequently brings new challenges to the effectiveness of current mainstream ART in China3. In Henan Province, a region with a
historical HIV burden linked to blood-selling practices in the 1990s, the epidemic has shifted to sexual transmission (92.78% in newly diagnosed HIV-1 infection)4. It is reported that about
10–30% of patients cannot effectively control their viral load (VL) after receiving standard ART5. Socioeconomic challenges, such as stigma and financial barriers to follow-up care, further
exacerbate suboptimal treatment outcomes6,7. Understanding the prevalence and drug resistance characteristics of this group and timely adjusting effective ART regimens have positive
significance for achieving the "95–95-95" goal and ending the AIDS epidemic by 20303. The overall incidence of acquired drug resistance mutations (DRMs) in PLWHA in China from 2001
to 2017 is about 44.7%8. According to the previous data of Henan Province, the incidence of DRMs in PLWHA with failed ART from 2018 to 2022 exceeded 80%9,10. This alarming rate underscores
the urgency of aligning treatment protocols with the WHO’s 2021 Consolidated Guidelines, which emphasize routine resistance testing and rapid transition to integrase strand transfer
inhibitors (INSTIs) like dolutegravir (DTG)11. While China has adopted DTG, its rollout in Henan is limited. Currently, research on DR mainly focuses on treatment-naive patients or PLWHA
with complete ART failure. However, more detailed research reveals that DR in other patient groups, like those with low-level viremia (LLV), cannot be overlooked. LLV refers to a relatively
low HIV-1 VL in the blood during ART (usually with a VL between 50 and 999 copies/mL)12. Apart from the facts that PLWHA with a VL < 1,000 copies/mL exhibit a reduced risk of transmitting
the infection as opposed to those with a VL of ≥ 1,000 copies/mL, further researches indicated that, relative to those with a VL of ≤ 50 copies/mL, individuals with LLV carry an increased
risk of ART failure13,14 and DR6,15. Given the significance of understanding the DR profiles in PLWHA with different levels of VL and its potential impact on ART effectiveness, in this
study, we specifically focused on PLWHA with detectable viremia (VL ≥ 40 copies/mL) after ART in Henan Province in 2023. By analyzing the distribution and drug resistance characteristics of
HIV-1 subtypes among them, we aim to provide valuable data to support for the clinical treatment and management of HIV-1, which is crucial for optimizing ART regimens and achieving better
treatment outcomes. RESULTS PATIENT CHARACTERISTICS A total of 987 PLWHA with detectable viremia after ART were included in this study. Samples from 804 patients were successfully genotyped,
giving a detection rate of 81.46%. Among the 804 successfully genotyped individuals, the median age was 49 years (IQR, 34–58), 73.51% (591/804) were male, 56.97% (458/804) were married, and
99.13% (797/804) were of Han ethnicity. The main route of transmission was sexual transmission (61.57%, 495/804), within which MSM accounted for 40.92% (329/804). Farmers accounted for
40.17% (323/804). According to the analysis, those with educational levels below junior college accounted for 68.28% (549/804). Detailed demographic characteristics of the patients are
presented in Table 1. GENOTYPE DISTRIBUTION The obtained _pol_ gene sequences were submitted to the REGA online HIV-1 subtype analysis tool for subtype analysis. Furthermore, a phylogenetic
tree was constructed based on the _pol_ gene sequences. All determined subtypes clustered with reference strains, indicating accurate subtype classification (Supplementary Fig. 1). A total
of 14 subtypes were detected. The subtype with the highest frequency was subtype B (55.97%, 450/804), followed by CRF01_AE (22.14%, 178/804), CRF07_BC (15.42%, 124/804), CRF55_01B (3.36%,
27/804), CRF08_BC (1.00%, 8/804), C (0.62%, 5/804), and other subtypes (1.49%, 12/804), including CRF67_01B (0.50%, 4/804), CRF62_BC (0.25%, 2/804), CRF02_AG (0.12%, 1/804), CRF03_A6B
(0.12%, 1/804), CRF52_01B (0.12%, 1/804), CRF59_01B (0.12%, 1/804), CRF68_01B (0.12%, 1/804), and G (0.12%, 1/804) (Table 2). CHARACTERISTICS OF DR Among 804 PLWHA with detectable viremia
after ART, 545 samples showed low-level or greater resistance to at least one ART drug, resulting in a total DR incidence of 67.79% (545/804). The prevalence of DR among PLWHA with the VL of
below and ≥ 200 copies/mL were 40.63% (13/32) and 68.91% (532/772), respectively (data not shown). Chi-squared analysis results indicated significant differences in DR incidence rates among
different subtypes (Table 2). Further analysis of DRMs revealed that NNRTIs-related mutations had the highest frequency (62.94%, 506/804), with mutation sites dominated by K103 (33.58%),
G190 (18.16%), V106 (17.91%), V179 (14.30%), and Y181 (14.05%). NRTIs-related mutations had a frequency of 53.23% (428/804), dominated by M184 (45.90%), K65 (19.28%), K70 (17.41%), S68
(16.04%), and D67 (11.94%). PIs-related mutations had a relatively low frequency of 7.34% (59/804), dominated by M46 (3.73%), V82 (3.23%), and I54 (2.86%). INSTIs-related mutations had the
lowest rate (3.98%, 32/804), dominated by E157 (1.37%), G163 (1.00%), and E138 (0.75%) (Fig. 1). Further analysis showed DRMs incidences: 20.90% (168/804) for single-class drugs, 45.77%
(368/804) for dual-class drugs, 6.47% (52/804) for triple-class drugs, and 0.37% (3/804) for quadruple-class drugs. Since over 90% of PLWHA in China were prescribed with free ART drugs,
namely abacavir (ABC), zidovudine (AZT), and lamivudine (3TC) of the NRTIs, tenofovir (TDF), efavirenz (EFV), and nevirapine (NVP) of the NNRTIs, and lopinavir/ritonavir (LPV/r) of the PIs,
we thus analyzed the DRMs against these seven drugs separately. The results showed that the prevalence of DRMs against the seven drugs is 65.30% (525/804), with ABC at 51.74% (416/804), AZT
at 14.43% (116/804), 3TC at 51.12% (411/804), TDF at 37.31% (300/804), EFV at 60.95% (490/804), NVP at 61.32% (493/804), and LPV/r at 4.85% (39/804). For individual drugs, NVP (60.32%,
485/804), EFV (55.22%, 444/804), and 3TC/emtricitabine (FTC) (45.77%, 368/804) showed the highest incidence of high-level resistance. Doravirine (DOR; 21.64%, 174/804), etravirine (ETR;
17.16%, 138/804), and TDF (17.04%, 137/804) have the highest incidence of medium-level resistance. Rilpivirine (RPV; 13.31%, 107/804), ABC (12.69%, 102/804), and TDF (9.95%, 80/804) have the
highest incidence of low-level resistance (Fig. 2). Detailed information on the drug resistance of ART drugs related to DRMs are presented in Fig. 2. ANALYSIS OF FACTORS INFLUENCING DRMS
Univariate logistic regression analysis found that patients aged 40–49 years old, baseline CD4 < 200 cells/µL, current VL of 103–105 copies/mL, current CD4 < 100 cells/µL, years of
infection ≥ 10 years, and those initially using the NRTI plus NNRTI ART regimen had a higher possibility of developing DR. Further multivariate logistic regression analysis showed that age
< 29 years old and 40–49 years old, baseline CD4 < 500 cells/µL, current VL of 103–105 copies/mL, and the initial ART regimen consisting of NRTI plus NNRTI only were closely related to
the occurrence of DR (Table 3). DISCUSSION Clarifying the occurrence of drug resistance at different VL levels is crucial for formulating personalized treatment plans and enhancing ART
effectiveness. In this study, we analyzed the genotype distribution and drug resistance characteristics of PLWHA with detectable viremia (VL ≥ 40 copies/mL) after six months of ART in Henan
Province in 2023, and our results provided critical insights for local HIV management. The high prevalence of DR (67.79%) highlights urgent challenges in Henan, where historical
blood-selling practices and current socioeconomic disparities (40.17% farmers, 68.28% education below junior college) drive suboptimal treatment outcomes. These factors lead to delayed
diagnosis, poor treatment adherence, and limited access to VL monitoring, all of which significantly exacerbate the DR risk7,16. Moreover, residual viremia, even at low levels (50–999
copies/mL), acts as a reservoir for continuous viral replication under the selective pressure of ART, and over time, this facilitates the accumulation of DRMs17,18. Notably, DR prevalence
among PLWHA with VL < 200 copies/mL was 40.63%, comparable to our previous data from Zhengzhou City (42.31% in 2022–2023) among low-level viremia (LLV) cases19, comfirming that LLV is not
negligible and requires proactive resistance testing beyond high VL cases. Compared with the prevalence of DR (about 80%) of PLWHA with ART failure in Henan Province from 2018 to 20229,10,
our findings (67.79%) reflect a moderate decrease but slightly higher than the survey data of Hainan Province from 2014 to 2020 (61.41%)20, Jilin Province from 2019 to 2021 (58.8%)21, and
Shanghai from 2017 to 2021 (48%)22. Our findings, when combined with those from other regions such as India (NNRTI and NRTI resistance rates of 73.13% and 68.83%, respectively)23 and
Tanzania24, highlight the global severity of the DR issue in HIV management. The data from these regions suggest that prolonged use of NNRTIs and NRTIs significantly raises the DR risk,
further emphasizing the need for treatment regimen optimization. Additionally, studies from Eastern Europe, Central Asia25 and Russia26 emphasize the importance of high genetic barrier
regimens like dolutegravir (DTG), in reducing DR. Our data, with a low INSTI resistance (3.98%), support WHO’s recommendation to shift to DTG-based regimens, especially in regions like Henan
where NNRTI resistance is high. Regional disparities in DR prevalence, for instance, Botswana (83.3%)27, Indonesia (22.1%)28, Suriname in South America (45.8%)29, underscore the need for
context-specific interventions tailored to local ART access and regimen choices. In this study, a total of 14 subtypes were detected. The predominance of subtype B (55.97%), followed by
CRF01_AE, CRF07_BC, mirrors historical Henan profiles9,10, but slightly differs from the subtype distribution characteristics reported in other regions of China21,22, and also different from
the subtype distribution characteristics of newly diagnosed PLWHA in Henan Province (mainly CRF07_BC subtype, followed by CRF01_AE, B, CRF55_01B and CRF08_BC)4,30, indicating different
subtype distribution characteristics in different regions and among different populations. This diversity implies that treatment policies cannot be generalized. When formulating treatment
strategies, local subtype distribution should be considered because different subtypes may respond differently to drugs, which can affect treatment outcomes. In 2023, among PLWHA with
detectable viremia, DRMs were predominantly in NNRTIs (62.94%, 506/804) and NRTIs (53.23%, 428/804). DRMs for PIs (7.34%, 59/804) and INSTIs (3.98%, 32/804) were relatively low, in line with
China’s ART regimens choices and the low DR barrier of NNRTIs drugs. The most common DRMs were NRTIs-related M184, K65, K70 and NNRTIs-related K103, G190, V106. M184 confers high-level
resistance to 3TC and FTC; K65 causes medium-level resistance to TDF, ABC, and 3TC/FTC, and is common in TDF/3TC regimen. K65R may increase sensitivity to AZT, but for INIST-naive patients
with K65R, TDF/3TC/DTG are more effective than AZT/3TC/DTG31,32. K70 leads to low-level resistance to ABC and TDF. Mutations at K103, G190, and V106 cause high-level resistance to NVP and
EFV33. Notably, DRMs related to PIs and INSTIs showed an upward trend compared to 2018–2022 (PIs: 7.34% vs. 5.2%; INSTIs: 3.98% vs. 3.1%)9. The most common PI mutation M46I/L reduces
susceptibility to ATV/r and LPV/r34. Among INSTIs mutations, minor mutations E157 and G163 predominated. A R263K mutation (0.50%) was identified, resulting an approximately two-fold
reduction in susceptibility to DTG, BIC, and CAB35. DRM profiles are crucial for accurate drugs selection, which can improve treatment success. Multivariate analysis indicated that age <
29 years and 40—49 years, baseline CD4 < 500 cells/µL, current VL of 103–105 copies/mL, and initial ART regimen of NRTI + NNRTI were closely associated with DR in PLWHA with detectable
viremia (Table 3). These populations require intensified monitoring and early initiation of WHO-recommended INSTI-based regimens to mitigate resistance accumulation. Expanding free
resistance testing to all detectable viremia cases, including LLV, and integrating DTG into first-line treatment are critical steps to align with global guidelines and address Henan’s unique
epidemic context. MATERIALS AND METHODS ETHICAL STATEMENT This study was approved by the Institutional Ethics Committee of The Sixth People’s Hospital of Zhengzhou, China
(IEC-KY-2022–005-2) and performed in compliance with all relevant ethical regulations such as the Declaration of Helsinki (2008). Signed informed consent was obtained from everyone before
the collection of blood samples. STUDY POPULATION From January to December 2023, PLWHA who visited the Sixth People’s Hospital of Zhengzhou, had received ART for more than 6 months, and had
a VL ≥ 40 copies/mL were included in this study. Demographic data and medical records of the patients, including HIV VL, CD4 + T-cell count, and transmission route, were collected. Informed
consent for participating in the study was obtained from the patients prior to sample collection. GENOTYPIC DRUG RESISTANCE TESTING The in-house genotypic drug resistance testing was carried
out as described in our previous studies35,36. Briefly, for patients with a viral load ≥ 400 copies/mL, whole blood was collected and centrifuged at low speed to obtain plasma. RNA was then
extracted using an RNA extraction kit (Liferiver, Shanghai, China) by following the manufacturer’s instructions. For those with a viral load < 400 copies/mL, 1–5 mL plasma was
ultracentrifuged at 28,000 g for 30 min at 4 °C to enrich HIV. The pellet was resuspended in phosphate buffered saline (0.01 M, pH 7.2) and used for RNA extraction. After that, the HIV-1
partial _pol_ and full-length integrase (INT) gene sequences were reverse-transcribed and amplified. Finally, the determined sequences were submitted to the regularly updated Stanford HIV-1
drug resistance database (http://hivdb.stanford.edu/) for analyses of drug resistance mutations (DRMs) and antiretroviral susceptibility. The estimated level of resistance to a drug is
determined by adding up the penalty scores associated with each of the DRMs present in a sequence. Once the total score is calculated the estimated level of resistance can be calculated as
follows: susceptible (total score 0 to 9); potential low-level resistance (total score 10 to 14); low-level resistance (total score 15 to 29); intermediate resistance (total score 30 to 59);
and high-level resistance (total score ≥ 60). Polymorphic mutations and polymorphic accessory mutations, when combined with other DRMs, may lead to reduced susceptibility to certain
antiretroviral drugs, so they are included in our analysis. The determined sequences have been deposited into the NCBI database, and the assigned accession numbers range from PV347152 to
PV347955. SUBTYPING AND PHYLOGENETIC ANALYSIS Subtyping and phylogenetic analyses were carried out as described previously. Briefly, the subtypes of HIV-1 isolates based on the partial _pol_
region was determined using the REGA HIV-1 Subtyping Tool (http://dbpartners.stanford.edu:8080/RegaSubtyping/stanford-hiv/typingtool/) and further confirmed by phylogenetic analysis.
Phylogenetic analysis was conducted using Molecular Evolutionary Genetic Analysis software (version XI), based on the maximum likelihood method and General Time Reversible model. Bootstrap
analysis with 1000 replicates was performed to test the tree topology. Reference sequences included in the ML tree (GenBank No. U51189, AF286226, AF286229, AF069670, AY945737, DQ207940,
U21135, AF067155, JX574661, AF077336, AF061642, AF190127, AF082395, AJ249235, AF286236) were downloaded from the Los Alamos HIV Sequence Database (https ://www.hiv.lanl.gov/). STATISTICAL
ANALYSIS Statistical analysis was carried out using SPSS 20.0 software. For continuous variables with a normal distribution, the mean ± standard deviation is employed. In the case of skewed
distributions, the median along with its interquartile range (from the first to the third quartile) is utilized. Categorical variables are presented as frequency or constituent ratio (%).
The t-test or chi-square test is used to analyze differences between groups. A two-sided test is conducted with a significant level of _α_ = 0.05. A _p_-value < 0.05 is considered
statistically significant. DATA AVAILABILITY The data used and analyzed in this study are available upon reasonable request. Please contact the corresponding author Yuqi Huo at
1246105,[email protected] to inquire about accessing the relevant datasets. We will review each request to ensure compliance with ethical and legal obligations and make every effort to provide the
data in a timely and appropriate manner. REFERENCES * Infectious Diseases Branch of Chinese Medical Association, A.a.H.C.G.C.C.f.D.C.a.P., _Chinese Guidelines for the Diagnosis and Treatment
of AIDS (2021 Edition). ._ Medical Journal of Peking Union Medical College Hospital. 13(02): p. 203–226 (2022). * Godfrey, C. et al. Global HIV Antiretroviral Drug Resistance: A Perspective
and Report of a National Institute of Allergy and Infectious Diseases Consultation. _J. Infect. Dis._ 216, S798–S800 (2017). Article PubMed PubMed Central Google Scholar * _The path
that ends AIDS: UNAIDS Global AIDS Update 2023. Geneva: Joint United Nations Programme on HIV/AIDS. (2023)._ Available at:
https://www.unaids.org/en/resources/documents/2023/global-aids-update-2023. (2023). * Liu, J., Liu, C., Wang, Y. _et al._, _Increased prevalence of pretreatment drug resistance mutations in
treatment-naïve people living with HIV-1 in Henan Province, China (2022/23)._ Infection, genetics and evolution. 115: p. 105520 (2023). * Hermans, L. E. et al. Effect of HIV-1 low-level
viraemia during antiretroviral therapy on treatment outcomes in WHO-guided South African treatment programmes: a multicentre cohort study. _Lancet Infect Dis._ 18(2), 188–197 (2018). Article
PubMed Google Scholar * Seth C, I., Silvia, B., Cissy M, K. _et al._, _The relative contributions of HIV drug resistance, nonadherence and low-level viremia to viremic episodes on
antiretroviral therapy in sub-Saharan Africa._ ADIS. 34(10): p. 1559–1566, (2020). * Momo Kadia, B.A.-O., Takah, N.F., Akem Dimala, C. & Smith, A., _Barriers to and enablers of uptake of
and adherence to antiretroviral therapy in the context of integrated HIV and tuberculosis treatment among adults in sub-Saharan Africa: a protocol for a systematic literature review._ BMJ
Open. (28;9(10):e031789). * Zuo, L., Liu, K., Liu, H. _et al._, _Corrigendum to "Trend of HIV-1 drug resistance in China: A systematic review and meta-analysis of data accumulated over
17 years (2001–2017)" [EClinicalMedicine 18 (2020) 100238]._ EClinicalMedicine. 33(100696) (2021). * Liu, J., Chen Z Fau - Wei, S., Wei S Fau - Ma, J. _et al._, _Drug resistance
mutations among people living with HIV with treatment failure in Henan Province, China._ Chin. Med. J. (Engl). 136(2542–5641) (2023). * Xuan, Y. et al. Characteristics of drug resistance in
HIV/AIDS patients with antiretroviral treatment failure in Henan Province. _Chinese J. Epidemiol._ 44(11), 1795–1801 (2023). Google Scholar * WHO, _Consolidated guidelines on HIV
prevention, testing, treatment, service delivery and monitoring._ (2021). * Olof, E. et al. All-Cause Mortality and Serious Non-AIDS Events in Adults With Low-level Human Immunodeficiency
Virus Viremia During Combination Antiretroviral Therapy: Results From a Swedish Nationwide Observational Study. _Clin. Infect Dis._ 72(12), 2079–2086 (2021). Article Google Scholar *
Appolonia, A., Sherri, P., Timothy, N. _et al._, _Retrospective longitudinal analysis of low-level viremia among HIV-1 infected adults on antiretroviral therapy in Kenya._ EClinicalMedicine.
63(0) (2023). * Mirriam M, N., Cecilia N, W., James M, K.e. & Nancy L M, B., _HIV Virologic Failure among Patients with Persistent Low-Level Viremia in Nairobi, Kenya: It Is Time to
Review the >1000 Virologic Failure Threshold._ .Biomed. Res. (2023). * Jinjin, L. et al. Characteristics of drug resistance mutations in ART-experienced HIV-1 patients with low-level
viremia in Zhengzhou City China. _Sci. Rep._ https://doi.org/10.1038/s41598-024-60965-z (2024). Article Google Scholar * Zhang, F. et al. Five-year outcomes of the China National Free
Antiretroviral Treatment Program. _Annals Internal Med._ 151(4), 241–251 (2009). Article Google Scholar * Hofstra, L. et al. Residual viremia is preceding viral blips and persistent
low-level viremia in treated HIV-1 patients. _PLoS ONE_ 9(10), e110749 (2014). Article ADS PubMed PubMed Central Google Scholar * Sahu, G. Potential implication of residual viremia in
patients on effective antiretroviral therapy. _AIDS Res. Hum. Retroviruses._ 31(1), 25–35 (2015). Article CAS PubMed PubMed Central Google Scholar * Liu, J. et al. Characteristics of
drug resistance mutations in ART-experienced HIV-1 patients with low-level viremia in Zhengzhou City China. _Sci. Rep._ 14(1), 10620 (2024). Article ADS CAS PubMed PubMed Central Google
Scholar * Yu, E. et al. HIV-1 Subtype Diversity and Factors Affecting Drug Resistance among Patients with Virologic Failure in Antiretroviral Therapy in Hainan Province, China, 2014–2020.
_Biomed. Environ. Sci._ 36(9), 800–813 (2023). CAS PubMed Google Scholar * Qi, G., Hui, W., Xihui, Z. _et al._, _Genotypic Drug Resistance Characteristics of HIV-1 Strains in HIV/AIDS
Patients with Failed Antiviral Therapy in Jilin Province_ Chinese Journal of Frontier Health and Quarantine. 46, 583–588, (2023). * Zhang, M. et al. The profile of HIV-1 drug resistance in
Shanghai, China: a retrospective study from 2017 to 2021. _J. Antimicrob Chemother._ 79(3), 526–530 (2024). Article CAS PubMed PubMed Central Google Scholar * Karade, S. et al. HIV drug
resistance following a decade of the free antiretroviral therapy programme in India: A review. _Int. J. Infect. Dis._ 66, 33–41 (2018). Article PubMed Google Scholar * Ntamatungiro, A.
et al. Strengthening HIV therapy and care in rural Tanzania affects rates of viral suppression. _J. Antimicrob. Chemother._ 72(7), 2069–2074 (2017). Article CAS PubMed Google Scholar *
Kirichenko, A. et al. Prevalence of HIV-1 drug resistance in Eastern European and Central Asian countries. _PLoS ONE_ 17(1), e0257731 (2022). Article CAS PubMed PubMed Central Google
Scholar * Kapustin, D. et al. Patterns of HIV-1 drug resistance among HIV-infected patients receiving first-line antiretroviral therapy in Novosibirsk Region Russia. _J. Glob. Antimicrobial
Resist._ 35, 1–5 (2023). Article CAS Google Scholar * Patrick T, M., Wonderful T, C., Dorcas, M. _et al._, _High prevalence of pre-treatment and acquired HIV-1 drug resistance mutations
among non-citizens living with HIV in Botswana._ Front Microbiol. https://doi.org/10.3389/fmicb.2024.1338191. (2024). * Nurjannah, Sri, J., Francisca Srioetami, T. _et al._, _Major Drug
Resistance Mutations on Reverse Transcriptase Gene in Human Immunodeficiency Virus Type-1 in Indonesia: A Systematic Review._ Curr. HIV/AIDS Rep. https://doi.org/10.1007/s11904-023-00687-5,
(2024). * Sno, R., Labadie-Bracho, M., Grünberg, M. & Adhin, M. First Assessment of Acquired HIV-1 Drug Resistance and Mutation Patterns in Suriname. _AIDS Res. Hum. Retro._ 37(7),
557–565 (2021). Article CAS Google Scholar * Liu, J. et al. Prevalence of transmitted drug resistance mutations among patients infected with human immunodeficiency virus type 1 (HIV-1) in
Henan Province China. _Chinese Med. J._ 135(22), 2750–2752 (2022). Article CAS Google Scholar * Paton, N. I. et al. Efficacy and safety of dolutegravir or darunavir in combination with
lamivudine plus either zidovudine or tenofovir for second-line treatment of HIV infection (NADIA): week 96 results from a prospective, multicentre, open-label, factorial, randomised,
non-inferiority trial. _Lancet HIV._ 9(6), e381–e393 (2022). Article CAS PubMed Google Scholar * Paton, N. I. et al. Dolutegravir or Darunavir in Combination with Zidovudine or Tenofovir
to Treat HIV. _N. Engl. J. Med._ 385(4), 330–341 (2021). Article CAS PubMed Google Scholar * Mazzuti, L. et al. Transmitted drug resistance mutations and trends of HIV-1 subtypes in
treatment-naïve patients: A single-centre experience. _J Glob Antimicrob. Resist._ 20, 298–303 (2019). Article PubMed Google Scholar * Kempf, D. J. et al. Identification of genotypic
changes in human immunodeficiency virus protease that correlate with reduced susceptibility to the protease inhibitor lopinavir among viral isolates from protease inhibitor-experienced
patients. _J. Virol._ 75(16), 7462–7469 (2021). * Yang, Z. et al. Prevalence of integrase strand transfer inhibitor (INSTIs) resistance mutations in Henan Province, China (2018–2020).
_Infection_ 49(6), 1195–1202 (2021). Article CAS PubMed Google Scholar * Yang, Z. et al. Characterization of HIV-1 subtypes and drug resistance mutations in Henan Province, China
(2017–2019). _Arch. Virol._ 165(6), 1453–1461 (2020). Article CAS PubMed PubMed Central Google Scholar Download references ACKNOWLEDGEMENTS We would like to thank all the doctors,
nurses, and patients who participated in this study. FUNDING This study was supported by the Science and Technology Project of Henan Province (232102310203). AUTHOR INFORMATION Author notes
* Jinjin Liu, Chaohong Fu and Xuan Yang contributed equally to this work. AUTHORS AND AFFILIATIONS * Affiliated Infectious Diseases Hospital of Zhengzhou University (Henan Infectious
Diseases Hospital, The SixthPeople’s Hospital of Zhengzhou), Erqi District, No.29, Jingguang South Road, Zhengzhou, 450000, China Jinjin Liu, Chaohong Fu, Xuan Yang, Xiaohua Zhang, Shuguang
Wei, Jie Ma, Qingxia Zhao & Yuqi Huo Authors * Jinjin Liu View author publications You can also search for this author inPubMed Google Scholar * Chaohong Fu View author publications You
can also search for this author inPubMed Google Scholar * Xuan Yang View author publications You can also search for this author inPubMed Google Scholar * Xiaohua Zhang View author
publications You can also search for this author inPubMed Google Scholar * Shuguang Wei View author publications You can also search for this author inPubMed Google Scholar * Jie Ma View
author publications You can also search for this author inPubMed Google Scholar * Qingxia Zhao View author publications You can also search for this author inPubMed Google Scholar * Yuqi Huo
View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS Yuqi Huo and Qingxia Zhao: Conceptualization, Methodology, Software, Validation, Data
curation, Visualization, Investigation. Jinjin Liu, Chaohong Fu, Xuan Yang, Xiaohua Zhang, Shuguang Wei and Jie Ma: Data curation, Investigation, Software, Validation. Jinjin Liu:
Visualization, Writing-original draft, review & editing. Yuqi Huo: Writing-review & editing. CORRESPONDING AUTHORS Correspondence to Qingxia Zhao or Yuqi Huo. ETHICS DECLARATIONS
COMPETING INTERESTS The authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER’S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps
and institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION. RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission
under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by
statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit
http://creativecommons.org/licenses/by-nc-nd/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Liu, J., Fu, C., Yang, X. _et al._ HIV-1 subtype distribution and drug
resistance profiles among PLWHA with detectable viremia in Henan Province, China, 2023. _Sci Rep_ 15, 17825 (2025). https://doi.org/10.1038/s41598-025-02949-1 Download citation * Received:
27 December 2024 * Accepted: 16 May 2025 * Published: 22 May 2025 * DOI: https://doi.org/10.1038/s41598-025-02949-1 SHARE THIS ARTICLE Anyone you share the following link with will be able
to read this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing
initiative KEYWORDS * Human immunodeficiency virus (HIV) * Antiretroviral therapy (ART) * Detectable viremia * Drug resistance (DR) * Subtype