Play all audios:
ABSTRACT STUDY DESIGN: Experimental, controlled, animal study. OBJECTIVES: To evaluate the effect of GM1 ganglioside, hyperbaric oxygen and both in combination, in the treatment of
experimental spinal cord lesions in rats. SETTING: Brazil. METHODS: Thirty-two Wistar rats with spinal cord lesions were divided into four groups: one group received GM1 ganglioside, one was
submitted to hyperbaric oxygen therapy (HBOT), the third received both treatments and the fourth received no treatment (control). RESULTS: There were no significant differences between the
groups in the histological analysis, for any of the variables (necrosis, hemorrhage, hyperemia, cystic degeneration, _P_>0.06). Neither were there any significant differences in the
comparison of left and right sides in the functional tests (_P_>0.06 for all). No significant differences were found in the locomotor ratings, in the comparison of groups at 2, 7, 21 and
28 days after the surgical procedure. However, in the evaluation on day 14, group 3, which received the combined therapy, showed a significantly higher Basso Beattie and Bresnahan score than
the other groups (_P_=0.015). CONCLUSION: The therapeutic effect of GM1 in locomotor evaluation of rats submitted to spinal cord lesion is anticipated by HBOT. SIMILAR CONTENT BEING VIEWED
BY OTHERS HYPERBARIC OXYGEN THERAPY IN CHILDREN WITH POST-CONCUSSION SYNDROME IMPROVES COGNITIVE AND BEHAVIORAL FUNCTION: A RANDOMIZED CONTROLLED TRIAL Article Open access 23 September 2022
RESHAPING CORTICAL CONNECTIVITY IN TRAUMATIC SPINAL CORD INJURY: A NOVEL EFFECT OF HYPERBARIC OXYGEN THERAPY Article Open access 09 September 2021 A DOUBLE-BLIND RANDOMIZED TRIAL OF
HYPERBARIC OXYGEN FOR PERSISTENT SYMPTOMS AFTER BRAIN INJURY Article Open access 26 February 2025 INTRODUCTION Totipotent, pluripotent or multipotent, autologous or homologous tissue and
stem cell growth factors have been tested in neuronal regeneration after spinal cord lesion. However, because of the short follow-up and evaluation period, there are still no concrete
results, and they remain as a future possibility for cure.1 The pharmacological therapies currently under investigation are calcium channel blockers, naloxones, gangliosides lazaroids,
dimethyl-sulfoxide and α-methylparatyrosine. Corticoids (particularly dexamethasone and methylprednisolone)2 and gangliosides, have already been protocoled for use in humans.
Methylprednisolone acts by decreasing cerebral edema and increasing blood flow, stabilizing the cell membrane and inhibiting lipid peroxidation, with a consequent decrease in the formation
of free radicals. A systematic review, published in 2000, showed that high doses of methylprednisolone are effective in the treatment of acute spinal cord lesion.3 GM1 (monosialoganglioside)
is a therapeutic option for the treatment of spinal cord injuries and injuries of the central nervous system.4, 5 Various properties are attributed to GM1, including a reduction in neuronal
edema by the increased activity of the sodium, potassium and magnesium pumps, homeostasis of the nerve cells by the reestablishment of membrane equilibrium, and in particular, the increase
of endogenous neurotrophic factors. This decreases neurone destruction after trauma, increasing the plasticity mechanisms of the injured spinal cord circuits and promoting the recovery of
functional connections.6 The analysis of the results of works involving GM1 in humans reveals an improvement in locomotor function,7 but the interpretation of these results is complex,
because of the fact that methylprednisolone was used before the administration of GM1.8 Hypothermia has been studied as a physical means of minimizing secondary spinal cord damage, with
beneficial effects when initiated in the first 8 h after trauma.9 However, its mortality rate is high.10 Another physical procedure that can be used is hyperbaric oxygen therapy (HBOT),11,
12 in which high partial pressures of tissue oxygen are obtained, which are higher than the atmospheric pressure. HBOT is based on the premise that a decrease in perfusion can be compensated
for by an increase in partial oxygen pressure. Experimental studies have been carried out that seek to elucidate the possible synergism between pharmacological factors of intervention in
spinal cord lesions.13 Similarly, it is possible that HBOT and GM1 have additive or synergic effects on spinal cord contusion injury. However, the effects of this treatment have still not
been clearly studied in spinal cord injury models. This study therefore seeks to evaluate, in a standardized experimental model, the influence of the treatment in rats submitted to acute
spinal cord injury with HBOT, monosialoganglioside (GM1) and a combination of both, on the functional and anatomopathological results. MATERIALS AND METHODS This is an experimental,
controlled trial on the use of GM1 ganglioside combined with HBOT in rats with induced spinal cord lesions. All applicable institutional and governmental regulations on the ethical use of
animals were followed during the course of this research. The research protocol was approved by the institution′s ethical committee. ANIMALS Young, adult, male Wistar rats were used,
weighing between 300 and 340 g, at 20–21 weeks of life, healthy and with normal motricity. All the animals were submitted to moderate spinal cord lesion, as described above.14 The 32 rats
were randomly separated into four groups, with eight animals in each: * Group 1: rats submitted to monosialoganglioside (GM1) treatment at a dose of 30 mg kg–1 for 7 days, starting 24 h
after the trauma; * Group 2: rats submitted to HBOT sessions with two ATM lasting 1 h, for 7 days, starting 24 h after the trauma; * Group 3: rats submitted to the combined therapy with GM1
and HBOT, according to the protocol applied in groups 1 and 2; * Group 4: rats not submitted to any treatment, serving as control. Rats that died after spinal cord lesion and those that
showed autophagic or mutilating behavior were excluded. Animals were also excluded that presented macroscopic spinal cord anomalies on surgery, or those that still presented normal movement
after the lesion (21 points on the Basso Beattie and Bresnahan (BBB) scale).15 At the end of the experimental period, all the rats were killed with a lethal dose of pentobarbital (140 mg
kg–1) per day, administered intraperitoneally. _Laminectomy._ All the rats received sodium pentobarbital anesthesia intraperitoneally (55–75 mg kg–1 body weight). The anesthetic took effect
after 5 min and lasted for at least 2 h. After anesthesia, the animals were trichotomized in the dorsal region and positioned on the surgical table. With the aid of an optical microscope, a
long, dorsal, medial incision was made in the skin and aponeurotic and muscular planes, to expose the posterior vertebral arches, from T8 to T12. The muscles inserted in the spinous process
and laminae of vertebrae T9 to T12 were undermined, and the joint processes of these vertebrae exposed. Hemostasia, wherein necessary, was performed using a bipolar coagulator. Using a bone
rongeur, the spinous process and laminae of vertebra T10 were removed, along with the distal half of the spinous process of T9, to expose the spinal cord and enable positioning (puncture) of
the tip of the NYU Impactor device, to perform the spinal cord lesion.13, 16 SPINAL CORD LESION The protocol for spinal cord lesion has been described elsewhere14 and consists of producing
a moderate spinal cord lesion with the NYU Impactor (New York University Spinal Cord Contusion System), a computerized device developed by New York University, which is designed to produce
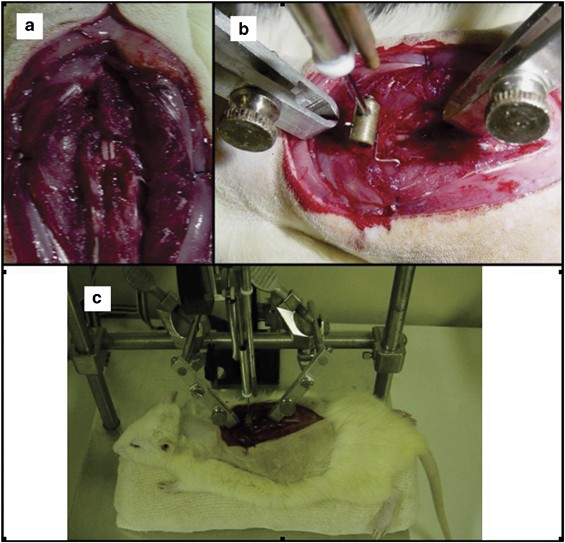
an impact using a falling weight. The impact was produced by the falling of an impact rod weighing 10 g, from a standardized height of 12.5 mm, compressing the spinal cord for 15 s. The
equipment allows the speed of the rod to be monitored by a computer, registering the exact moment the rod makes contact with the spinal cord and the length of time of the contact, using
spine motion sensors (Figure 1). The animals were positioned so that NYU Impactor rod touched the exposed spinal cord at vertebra T10. This was carried out by fixing the T8 and T11 spinous
processes using two clamps, fastened to the base of the NYU Impactor. This ensured that the lesions were homogenous and reproducible. The site of the contusion injury was inspected. Where
hemorrhaging was present, hemostasia was performed. The contusion site was then washed with physiological sodium chloride solution at room temperature. The muscle, fascia and skin tissue
planes were closed by simple suture stitches, using 2.0 monofilament nylon. _Postoperative procedures._ After producing the lesions, the animals were placed under a heat source at a
temperature of 25–28 °C. The rats’ bladders were pressed, to empty them. Once they had recovered from the anesthesia, the animals were allowed food and water. The animals then received
cephalothin (Keflin Neutro, Ely Lilly, Brazil) subcutaneously (25 mg kg–1 body weight, once a day, for 7 days) immediately after the lesion, and once a day for the next 7 days, to prevent
urinary tract or wound infection. Those that presented infection received the antibiotic for 10 days, and were excluded from the statistical analysis. HYPERBARIC OXYGEN THERAPY HBOT was
applied at two ATM for 1 h day–1 (after equalizing the pressure) for seven consecutive days.11, 12 A tubular hyperbaric chamber was used, measuring 770 mm in length and 180 mm in internal
diameter, with a useful height of 150 mm (between the platform and the upper wall), transparent, acrylic walls of 10 mm in thickness and capacity to hold 10 rats simultaneously. The
hyperbaric chamber was regulated to provide 14 l of oxygen per minute. PROTOCOL FOR EVALUATING LOCOMOTOR CAPACITY The recovery of locomotor capacity after spinal cord lesion was measured by
the BBB scale of functional evaluation,15 applied with simultaneous visual evaluation by two trained observers, who had no knowledge of the intervention to which each rat had been submitted
(that is, they were blind to the procedure). The evaluation, carried out on days 2, 7, 13, 21 and 28 after surgery, was made by consensus or, in the case of a disagreement, the lowest value
was recorded. The experimental murine spinal cord lesion evaluation model of the MASCIS (Multicenter Animal Spinal Cord Injury Study) was adopted, standardized for Wistar rats.17 The
following indicators were observed and recorded: joint movements of the hind paw, trunk and abdomen position, dislocation of the paw and type of contact of the paw with the ground, toe
coordination, contact and lifting the paw from the ground, trunk instability, and tail position in relation to the right and left sides. If the rat remained immobile for 15–20 s, movement
was stimulated by touching the animal. The evaluation took 4–5 min. NECROSCOPIC AND ANATOMOPATHOLOGICAL EXAM In the initial necroscopic inspection, the presence of possible lesions
associated with autophagia or mutilation was observed. The internal inspection was begun by removing the vertebral column, making a new extensive dorsal incision, exposing the spine and
cutting a segment from T8 to T12 using scissors. Using a micro bone rongeur, all the bone structures were carefully removed, as well as the soft parts adjacent to the spinal cord, to expose
it completely. Visual macroscopic evaluation of the spinal cord at the contusion site was carried out, to check for any anomaly (exclusion criteria). Ventral incision (thoracotomy and
laparotomy) was performed, to inspect the lungs, abdomen and bladder, looking for signs of empyema, condensation, flaccid neurogenic bladder (with increase in volume) or hyperemia and
hematuria. Next, the spinal cord, preserved in 10% formaldehyde solution, was sent for microscopic (optical) analysis. Histological cross-sections were made on the axial plane in the spinal
cord segment, at 2 mm intervals, representing the entire lesioned area, to a length of 1 cm from the center of the lesion. This material was processed and dehydrated in a series of alcohols,
then diaphanized in xylol and embedded in paraffin. Five-micra thick histological sections were produced in a microtome, half a centimeter above and half a centimeter below the central area
of the lesion. The material was then fixed on glass slides stained with hematoxylin-eosin. Three slides were prepared for each spinal cord, denominated A, B and C. Slides A and C
corresponded to the proximal and distal regions of the site of the lesion, respectively, and were collected as a form of individual control in each rat. Fragment B corresponded to the site
of the lesion itself. All the fragments were graded for necrosis, hemorrhage, hypermia, degeneration of nervous substances (cystic degeneration) and cell infiltration, as absent (0), slight
(1), moderate (2) and accentuated (3). The pathologists were not informed of the group of origin to which the rat spinal cord belonged (blind evaluation). STATISTICAL ANALYSIS Owing to the
nature of the variables, non-parametric tests were used. The Kruskal–Wallis test was used to compare the study groups, in terms of BBB score for each evaluation time, as well as for the
distribution of anatomical–pathological analysis scores. The differences between the groups, wherein significant, were determined by Dunn's multiple comparison test. The comparison of
mortality between the groups was performed by the _χ_2 and verisimilitude ratio tests. _P-_values of <0.05 were considered significant. RESULTS Table 1 shows the deaths and causes of
death among the animals studied, none of which was related to the procedure itself. There was no difference between the groups, in relation to mortality (_P_=0.908). Table 1 shows that only
one animal was excluded because of autophagia. There were no cases of mutilation, spinal cord macroscopic anomalies or normal movements after the spinal cord lesion (reasons that would
justify further exclusions). There were no significant differences between the groups in the histological analysis, regardless of the variable (necrosis, hemorrhage, hyperemia, cystic
degeneration, _P_>0.06) or region, A, B or C, being considered. Neither were there any significant differences in the comparison of left and right sides in the functional tests
(_P_>0.06 for all). No significant difference was found in locomotor ratings in the comparison of groups at 2, 7, 21 or 28 days after the surgical procedure. However, in the evaluation on
day 14, group 3, which received the combined therapy, showed a significantly higher BBB score than the other groups (_P_=0.015, Table 2). DISCUSSION Combining a physical medium (HBOT) with
a pharmacological method (GM1) for the treatment of spinal cord lesions, this is the first time an attempt has been made to potentialize the effects of both. The treatment can be evaluated
both in terms of functional aspects (recovery of movements) and histological aspects. As expected, in this study, there was no statistically significant difference in the results of the
anatomopathological analysis with the application of each treatment in isolation, or both in combination. The low sensitivity of the hematoxylin-eosin staining method could explain the
difficulty in detecting possible differences between the groups. The use of a lesion grading of 12.5 mm in height, which is smaller than that used in the majority of the other studies, may
also have influenced the result. The locomotor capacity of group 3 (which received HBOT and GM1) was significantly higher than that of the other groups in the second week of the analysis.
However, in the subsequent weeks, the treatment groups and the control did not show any statistical differences between them. These results show that the use of GM1 caused a beneficial
effect in the functional recovery of the rats, which appears to have been potentialized by the use of hyperbaric oxygen in the second week after lesion. The small sample or insufficient
follow-up time may explain the lack of statistical support. Even so, hyperbaric oxygenation appears to have momentarily accelerated recovery (group 3 in the second week) caused by the
pharmacological therapy, while hyperbaric oxygen used in isolation (group 2) did not cause any benefit. It is worth discussing whether the time of use of the HBOT should not have been
greater than that used. In experiments with animal models, various application times of the HBOT were used, from 15 min after the lesion,12 to 218 to 4 h.19 In humans, it is recommended20
that hyperbaric therapy be initiated within 4 h of the spinal cord lesion. In this study, the start of therapy in the hyperbaric chamber occurred 24 h after the spinal cord model lesion was
produced in the animals, and it is possible that the effects of HBOT would be more intense if administrated earlier, a possibility that should be investigated in future studies. Other
studies12, 18, 19, 21 use oxygen under pressure at two–five ATA in animals submitted to induced spinal cord lesion. Above these pressures, the side effects, such as necrosis of the cells of
the anterior horn of the spinal cord in rats, or enzyme degradation by oxidation in the brain, may occur.22 Although there is no precise and definitive data on the ideal pressure for
experimentation in rats, this study opted for a pressure of two ATA.11, 19 The National Acute Spinal Cord Injury Studies (NASCIS-2 and NASCIS-3) protocol, which is widely used, results in an
improvement in neurological function in acute spinal cord lesion. Gangliosides (GM1) have shown a neurotrophic effect, but appear to inhibit the neuroprotective effects of the
methylprednisolone and its mechanism of action, although this is not well elucidated, and this drug is still in the experimental stage.5, 13 It is observed that in clinical practice, the use
of drugs is restricted to a coadjuvant action in acute spinal cord injury, and more evidence is required of its mechanism of action and effectiveness. This experimental research offers
evidence that there appears to be a beneficial effect in the use of GM1 in the functional recovery in spinal cord lesion, an effect that is potentialized through the combination of GM1 and
HBOT. CONCLUSIONS The therapeutic effect of GM1 on the motricity of Wistar rats submitted to spinal cord lesion is anticipated, through the use of HBOT. REFERENCES * Cristante AF,
Barros-Filho TE, Tatsui N, Mendrone A, Caldas JG, Camargo A _et al_. Stem cells in the treatment of chronic spinal cord injury: evaluation of somatosensitive evoked potentials in 39
patients. _Spinal Cord_ 2009; 47: 733–738. Article CAS PubMed Google Scholar * Bracken MB, Shepard MJ, Collins Jr WF, Holford TR, Baskin DS, Eisenberg HM _et al_. Methylprednisolone or
naloxone treatment after acute spinal cord injury: 1-year follow-up data. Results of the second National Acute Spinal Cord Injury Study. _J Neurosurg_ 1992; 76: 23–31. Article CAS PubMed
Google Scholar * Bracken MB . Pharmacological interventions for acute spinal cord injury. _Cochrane Database Syst Rev_ 2000: (2). Art. no. CD001046. * Walker JB, Harris M . GM1 ganglioside
administration combined with physical therapy restores ambulation in humans with chronic spinal cord injury. _Neurosci Lett_ 1993; 161: 174–178. Article CAS PubMed Google Scholar *
Geisler FH, Dorsey FC, Coleman WP . Recovery of motor function after spinal-cord injury—a randomized, placebo-controlled trial with GM1 ganglioside. _N Engl J Med_ 1991; 324: 1829–1838.
Article CAS PubMed Google Scholar * Cuello AC, Garofalo L, Kenigsberg RL, Maysinger D . Gangliosides potentiate _in vivo_ and _in vitro_ effects of nerve growth factor on central
cholinergic neurons. _Proc Natl Acad Sci USA_ 1989; 86: 2056–2060. Article CAS PubMed PubMed Central Google Scholar * Geisler FH, Coleman WP, Grieco G, Poonian D, Sygen Study Group. The
Sygen multicenter acute spinal cord injury study. _Spine (Phila Pa1976)_ 2001; 26 (24 Suppl): S87–S98. Article CAS Google Scholar * Blight AR, Zimber MP . Acute spinal cord injury:
pharmacotherapy and drug development perspectives. _Curr Opin Investig Drugs_ 2001; 2: 801–808. CAS PubMed Google Scholar * Albin MS, White RJ . Epidemiology, physiopathology, and
experimental therapeutics of acute spinal cord injury. _Crit Care Clin_ 1987; 3: 441–452. Article CAS PubMed Google Scholar * Schwab ME, Bartholdi D . Degeneration and regeneration of
axons in the lesioned spinal cord. _Physiol Rev_ 1996; 76: 319–370. Article CAS PubMed Google Scholar * Shiokawa O, Fujishima M, Yanai T, Ibayashi S, Ueda K, Yagi H . Hyperbaric oxygen
therapy in experimentally induced acute cerebral ischemia. _Undersea Biomed Res_ 1986; 13: 337–344. CAS PubMed Google Scholar * Murakami N, Horinouchi T, Sakurai M, Ejima Y, Matsukawa S,
Kato M _et al_. Hyperbaric oxygen therapy given 30 min after spinal cord ischemia attenuates selective motor neuron death in rabbits. _Crit Care Med_ 2001; 29: 814–818. Article CAS PubMed
Google Scholar * Constantini S, Young W . The effects of methylprednisolone and the ganglioside GM1 on acute spinal cord injury in rats. _J Neurosurg_ 1994; 80: 97–111. Article CAS
PubMed Google Scholar * Narazaki DK, Barros Filho TE, Oliveira CR, Cristante AF, Iutaka AS, Marcon RM _et al_. Spinal cord regeneration: the action of neurotrophin-3 in spinal cord injury
in rats. _Clinics (Sao Paulo)_ 2006; 61: 453–460. Article Google Scholar * Basso DM, Beattie MS, Bresnahan JC . A sensitive and reliable locomotor rating scale for open field testing in
rats. _J Neurotrauma_ 1995; 12: 1–21. Article CAS PubMed Google Scholar * New York University, Medical Center. Impactor. NYU spinal cord contusion system. Operation Manual. Impactor
Software Version 7.0., New York, 1993, 41p. * Basso DM, Beattie MS, Bresnahan JC, Anderson DK, Faden AI, Gruner JA _et al_. MASCIS evaluation of open field locomotor scores: effects of
experience and teamwork on reliability. Multicenter animal spinal cord injury study. _J Neurotrauma_ 1996; 13: 343–359. Article CAS PubMed Google Scholar * Higgins AC, Pearlstein RD,
Mullen JB, Nashold Jr BS . Effects of hyperbaric oxygen therapy on long-tract neuronal conduction in the acute phase of spinal cord injury. _J Neurosurg_ 1981; 55: 501–510. Article CAS
PubMed Google Scholar * Kelly Jr DL, Lassiter RL, Vongsvivut A, Smith JM . Effects of hyperbaric oxygenation and tissue oxygen studies in experimental paraplegia. _J Neurosurg_ 1972; 36:
425–429. Article PubMed Google Scholar * Gamache Jr FW, Myers RA, Ducker TB, Cowley RA . The clinical application of hyperbaric oxygen therapy in spinal cord injury: a preliminary report.
_Surg Neurol_ 1981; 15: 85–87. Article PubMed Google Scholar * Balentine JD . Central necrosis of the spinal cord induced by hyperbaric oxygen exposure. _J Neurosurg_ 1975; 43: 150–155.
Article CAS PubMed Google Scholar * Balentine JD . Dendritic degeneration following hyperbaric oxygen exposure. _Adv Neurol_ 1975; 12: 471–481. CAS PubMed Google Scholar Download
references ACKNOWLEDGEMENTS There was no funding for the study. The drug studied (GM1) was donated by TRB Pharma Laboratory. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of
Orthopaedics and Traumatology, University São Paulo Medicine School, São Paulo, Brazil R M Marcon, A F Cristante, T E P de Barros Filho, R P de Oliveira & G B dos Santos Authors * R M
Marcon View author publications You can also search for this author inPubMed Google Scholar * A F Cristante View author publications You can also search for this author inPubMed Google
Scholar * T E P de Barros Filho View author publications You can also search for this author inPubMed Google Scholar * R P de Oliveira View author publications You can also search for this
author inPubMed Google Scholar * G B dos Santos View author publications You can also search for this author inPubMed Google Scholar CORRESPONDING AUTHOR Correspondence to R M Marcon. ETHICS
DECLARATIONS COMPETING INTERESTS The authors declare no conflict of interest. RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Marcon, R., Cristante, A.,
de Barros Filho, T. _et al._ Potentializing the effects of GM1 by hyperbaric oxygen therapy in acute experimental spinal cord lesion in rats. _Spinal Cord_ 48, 808–813 (2010).
https://doi.org/10.1038/sc.2010.37 Download citation * Received: 20 October 2009 * Revised: 19 February 2010 * Accepted: 05 March 2010 * Published: 27 April 2010 * Issue Date: November 2010
* DOI: https://doi.org/10.1038/sc.2010.37 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative KEYWORDS * hyperbaric oxygenation * G(M1) ganglioside * spinal
cord injuries