Play all audios:
Basal cell carcinoma (BCC) is the most common malignant eyelid tumour. Although it may be treated by external beam radiotherapy, severe radiation retinopathy in this setting is extremely
rare.1
A 39-year-old lady was successfully treated with 45 Gray (Gy) of external beam radiotherapy in nine equal fractions for a lateral lower lid BCC. An internal eye shield was used to protect
the globe. After 8 years, her optometrist referred her to the local eye clinic after finding abnormal peripheral retinal blood vessels. After excluding diabetes and hypertension, radiation
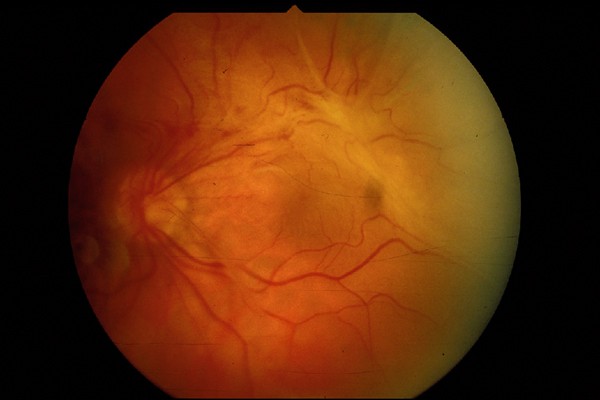
retinopathy was diagnosed. The patient subsequently experienced recurrent small vitreous haemorrhages. After 4 years, there were signs of proliferative radiation retinopathy including a
macular-threatening tractional retinal detachment, reducing visual acuity to less than 6/60 (see Figure 1).
The patient underwent indirect two-port vitrectomy, membrane delamination, encircling band and silicone oil tamponade. Visual acuity, after removal of silicone oil, improved to 6/24 and has
remained stable for 3 years. Histology demonstrated blood vessels within the excised membrane (see Figure 2). The membrane was indistinguishable from those excised from patients with the
late complications of proliferative diabetic retinopathy.
Haematoxylin-and-eosin-stained section showing a portion of the paucicellular epiretinal membrane in which several capillaries can be seen (original magnification × 400).
A large study looking at radiation retinopathy after external beam radiotherapy for extracranial head and neck tumours showed that, in the absence of other risk factors, it was only seen at
total doses above 45 Gy.2 The risk of radiation retinopathy increased with higher total dose. Dose fractions of greater than 1.9 Gy increased the risk of radiation retinopathy when the total
dose was in the range of 45–55 Gy.
Although epiretinal membranes are relatively common, they are only rarely caused by proliferative radiation retinopathy.3 This type of epiretinal membrane is frequently treatable by
vitrectomy.4 This is likely to require division of vascular bridges either with scissors or blunt dissection for successful completion of the delamination.
This report highlights a previously rarely reported and potentially sight-threatening complication in the treatment of eyelid BCC. The clinicopathological differences compared with other
more common causes of epiretinal membrane have important implications for the surgical approach.
Anyone you share the following link with will be able to read this content: